Yücel Murat, Uğuz Emrah, Erdoğan Kemal Eşref, Şener Erol
Department of Cardiovascular Surgery, Ankara Bilkent City Hospital, 06800 Ankara, Türkiye.
Department of Cardiovascular Surgery, Ankara Yıldırım Beyazıt University Faculty of Medicine, 06010 Ankara, Türkiye.
J Clin Med. 2025 Mar 26;14(7):2248. doi: 10.3390/jcm14072248.
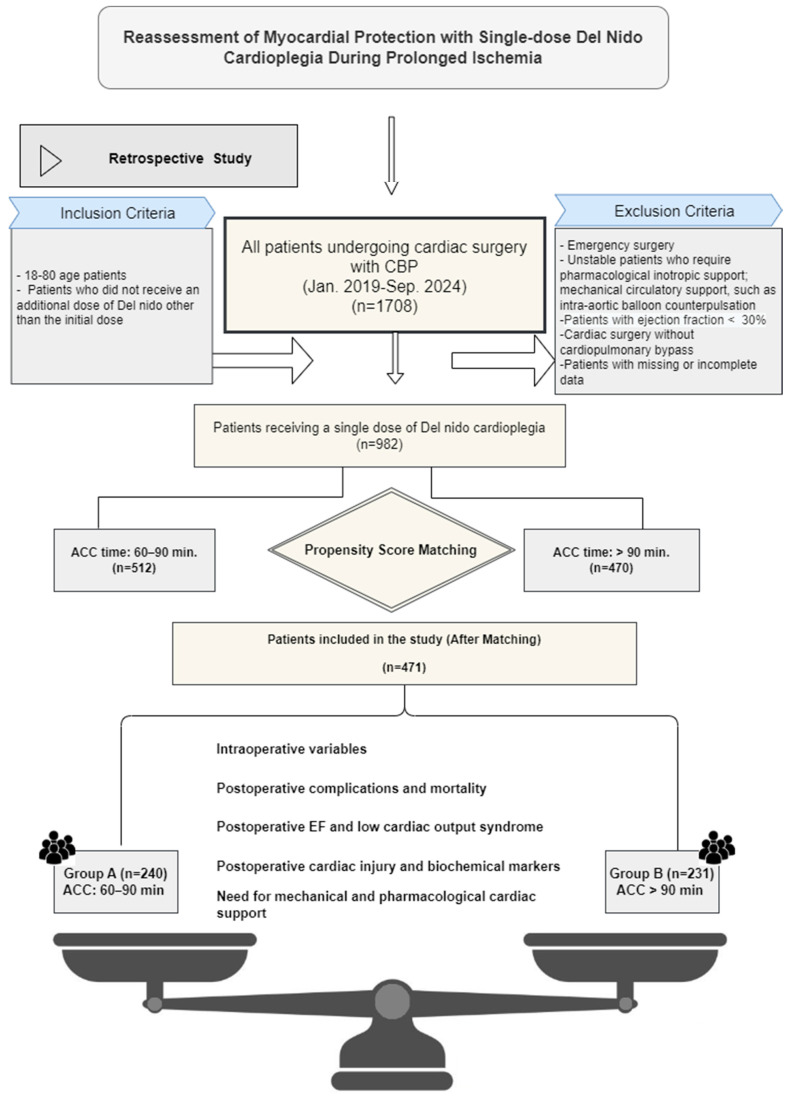
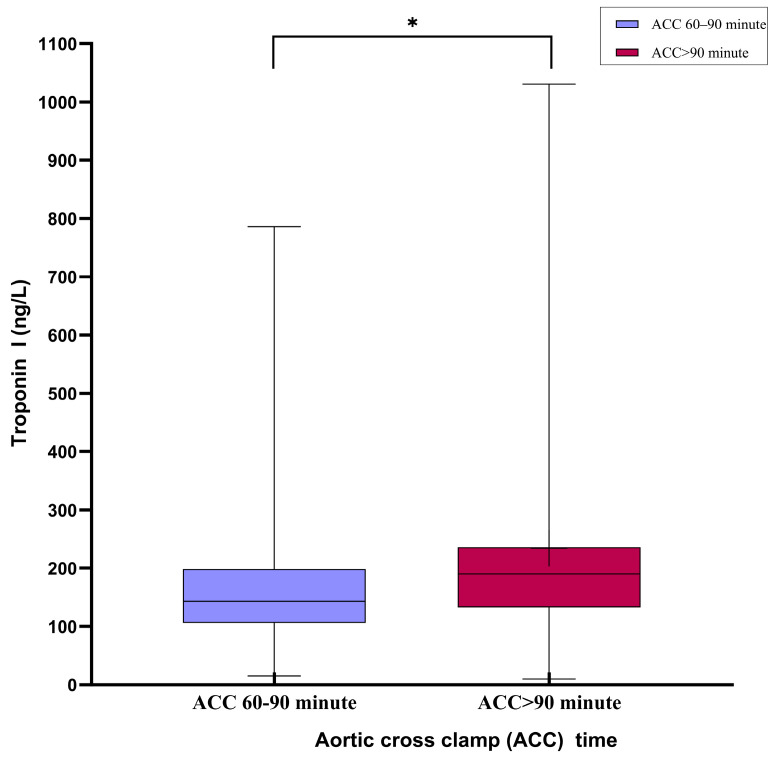
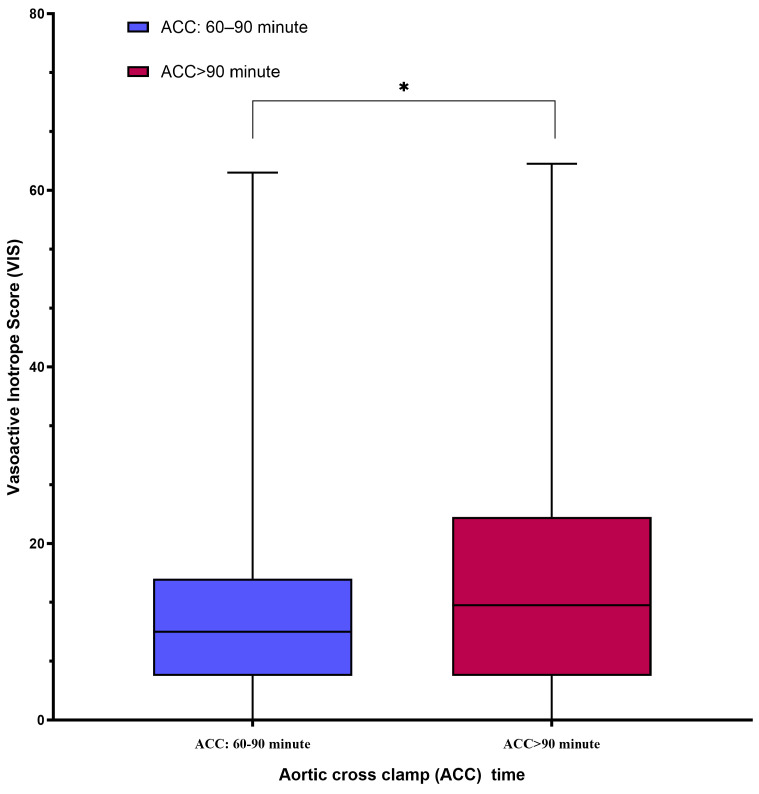
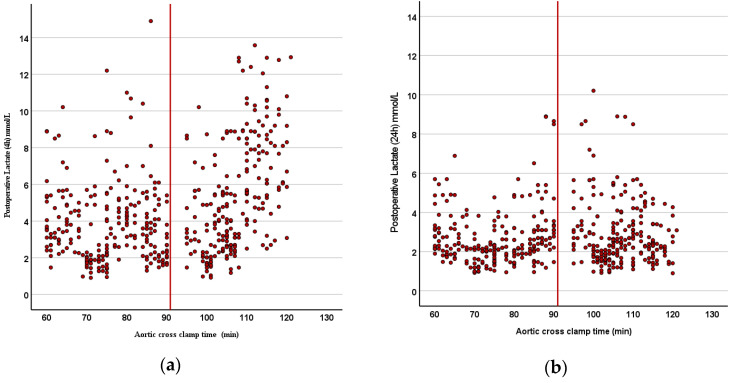
Del Nido (DN) cardioplegia is widely used in cardiac surgery for its efficacy in providing myocardial protection for up to 90 min with a single dose. However, its safety and efficacy during prolonged ischemia remain unclear. This retrospective study analyzed 471 patients who underwent cardiac surgery with CPB between January 2019 and September 2024. Patients were divided into two groups: ACC durations of 60-90 min (Group A, n = 240) and >90 min (Group B, n = 231). The perioperative characteristics, clinical outcomes, and biochemical markers were compared to evaluate the impact of prolonged ischemia. Patients in Group B exhibited significantly higher postoperative troponin I and lactate levels at 4 h post-CPB, suggesting increased myocardial and metabolic stress. Lactate levels normalized within 24 h, indicating transient myocardial dysfunction. Defibrillation requirements and vasoactive inotropic score (VIS) were also significantly elevated in Group B, reflecting compromised myocardial electrical stability and hemodynamic challenges. However, the long-term outcomes such as mortality, LCOS, and MODS showed no significant differences between the groups. While DN cardioplegia provides sufficient myocardial protection for ACC durations within 90 min, its efficacy diminishes during prolonged ischemia, as evidenced by increased myocardial injury and hemodynamic instability. Tailored strategies, including standardized redosing protocols and enhanced perioperative management, are essential for optimizing outcomes in complex surgeries with extended ischemia times. Further prospective studies are needed to refine these protocols and assess alternative solutions for myocardial protection.
德尔尼多(DN)心脏停搏液因其单次给药能为心肌提供长达90分钟的有效保护,而在心脏手术中被广泛应用。然而,其在长时间缺血期间的安全性和有效性仍不明确。这项回顾性研究分析了2019年1月至2024年9月期间接受体外循环心脏手术的471例患者。患者被分为两组:主动脉阻断时间为60 - 90分钟(A组,n = 240)和>90分钟(B组,n = 231)。比较围手术期特征、临床结局和生化指标,以评估长时间缺血的影响。B组患者在体外循环后4小时的术后肌钙蛋白I和乳酸水平显著升高,提示心肌和代谢应激增加。乳酸水平在24小时内恢复正常,表明存在短暂的心肌功能障碍。B组的除颤需求和血管活性药物评分(VIS)也显著升高,反映出心肌电稳定性受损和血流动力学挑战。然而,两组之间的长期结局如死亡率、住院时间延长(LCOS)和多器官功能障碍综合征(MODS)并无显著差异。虽然DN心脏停搏液在90分钟内的主动脉阻断时间能提供足够的心肌保护,但其在长时间缺血期间的疗效会降低,这表现为心肌损伤增加和血流动力学不稳定。包括标准化再给药方案和加强围手术期管理在内的定制策略,对于优化缺血时间延长的复杂手术的结局至关重要。需要进一步的前瞻性研究来完善这些方案,并评估心肌保护的替代解决方案。