Zhao Yaoping, Yu Shuang, Zhang Dong, Zheng Shaoqiang, Cai Nan, Zhang Qiang, Wang Geng
Department of Anesthesiology, Beijing Jishuitan Hospital, Capital Medical University, Xinjiekou No. 31 East Street, Xicheng District, Beijing, 100035, China.
Department of Anesthesiology, Aerospace Central Hospital, Beijing, 100049, China.
J Cardiothorac Surg. 2025 Apr 17;20(1):207. doi: 10.1186/s13019-025-03437-3.
To evaluate the impact of preoperative pleural effusion on the ultrasound visualization of the paravertebral space (PVS), thoracic paravertebral nerve block administered by anesthesiologists, and to investigate whether ultrasound combined with pressure guidance can assist in locating the paravertebral space in patients with pleural effusion.
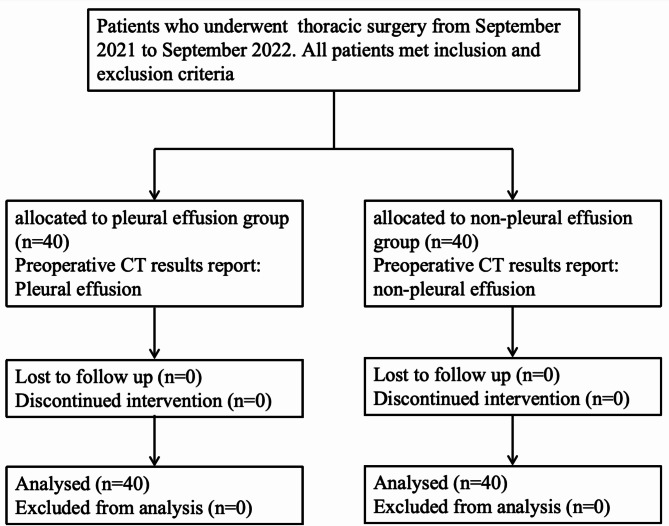
This prospective observational study enrolled patients undergoing thoracic surgery at Beijing Jishuitan Hospital between September 2021 and September 2022. Patients were categorized into two groups based on preoperative CT findings: the pleural effusion group (n = 40) and the non-pleural effusion group (n = 40). Prior to the induction of general anesthesia, all patients were placed in a lateral position. Thoracic paravertebral nerve block (TPVB) was administered using ultrasound guidance combined with pressure monitoring, with a 20 ml of 0.5% ropivacaine.
Parameters recorded included the duration of puncture and ultrasound pre-scan for TPVB, the ultrasound image definition score of the PVS, the pressure in the external intercostal muscle and PVS, and additional relevant indicators. Mean arterial pressure (MAP) and heart rate (HR) were measured before anesthesia induction, post-induction, and during skin incision. Compared to the non-pleural effusion group, the pleural effusion group demonstrated prolonged ultrasound pre-scan and puncture durations. The PVS definition score, the ventral displacement of the pleura, and the accuracy of resident anesthesiologists in identifying the PVS were all significantly lower in the pleural effusion group (p < 0.05). Compared to non-pleural effusion group, the pleural effusion group had significantly higher pressure in PVS. In the pleural effusion group, the pressure in PVS was significantly lower than that in external intercostal muscle (p < 0.05). No significant differences were observed in MAP and HR between the two groups before anesthesia induction, post-induction and during skin incision (p > 0.05).
Preoperative pleural effusion is associated with reduced clarity of ultrasound visualization of the PVS, and extended procedural durations for anesthesiologists, thereby increasing the complexity of TPVB. Pressure detection during TPVB implementation can assist in locating the position of the puncture needle. For anesthesiologists with less experience, TPVB should be carefully performed in patients with preoperative pleural effusion.
The trial was prospectively registered with the Chinese Clinical Trial Registry under registration number ChiCTR2100050582, on August 30, 2021.
评估术前胸腔积液对椎旁间隙(PVS)超声可视化的影响、麻醉医生实施胸椎椎旁神经阻滞的情况,并研究超声联合压力引导能否辅助定位胸腔积液患者的椎旁间隙。
本前瞻性观察性研究纳入了2021年9月至2022年9月在北京积水潭医院接受胸外科手术的患者。根据术前CT检查结果将患者分为两组:胸腔积液组(n = 40)和无胸腔积液组(n = 40)。在全身麻醉诱导前,所有患者均取侧卧位。采用超声引导联合压力监测,给予20 ml 0.5%的罗哌卡因进行胸椎椎旁神经阻滞(TPVB)。
记录的参数包括TPVB的穿刺时间和超声预扫描时间、PVS的超声图像清晰度评分、肋间外肌和PVS内的压力以及其他相关指标。在麻醉诱导前、诱导后和皮肤切开时测量平均动脉压(MAP)和心率(HR)。与无胸腔积液组相比,胸腔积液组的超声预扫描和穿刺时间延长。胸腔积液组的PVS清晰度评分、胸膜腹侧移位以及住院麻醉医生识别PVS的准确性均显著降低(p < 0.05)。与无胸腔积液组相比,胸腔积液组的PVS内压力显著更高。在胸腔积液组中,PVS内压力显著低于肋间外肌内压力(p < 0.05)。两组在麻醉诱导前、诱导后和皮肤切开时的MAP和HR均无显著差异(p > 0.05)。
术前胸腔积液与PVS超声可视化清晰度降低以及麻醉医生操作时间延长相关,从而增加了TPVB的复杂性。在TPVB实施过程中进行压力检测有助于定位穿刺针位置。对于经验较少的麻醉医生,在术前有胸腔积液的患者中应谨慎实施TPVB。
该试验于2021年8月30日在中国临床试验注册中心进行前瞻性注册,注册号为ChiCTR2100050582。