Mazzeo Pierluigi, Ceccato Filippo, Tizianel Irene, Barbot Mattia
Department of Medicine DIMED, Endocrine Unit, University of Padova, Padua, Italy.
Endocrine Unit, University Hospital of Padova, Padua, Italy.
Case Rep Endocrinol. 2025 Apr 11;2025:1422782. doi: 10.1155/crie/1422782. eCollection 2025.
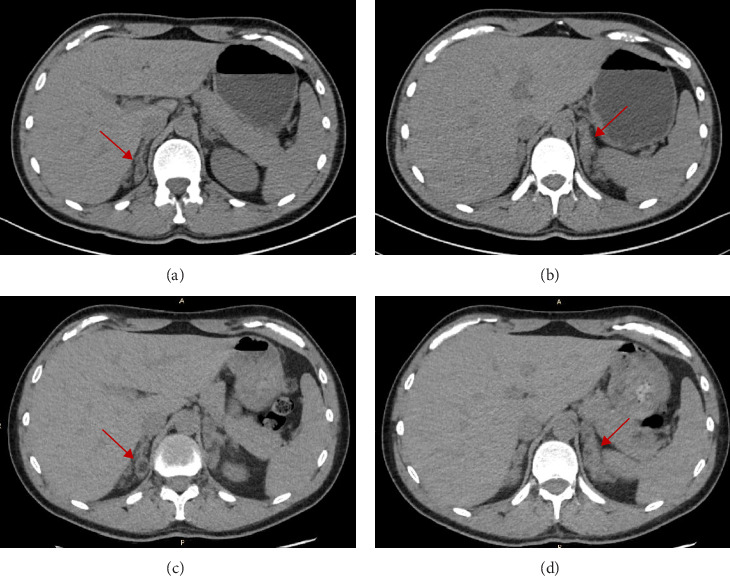
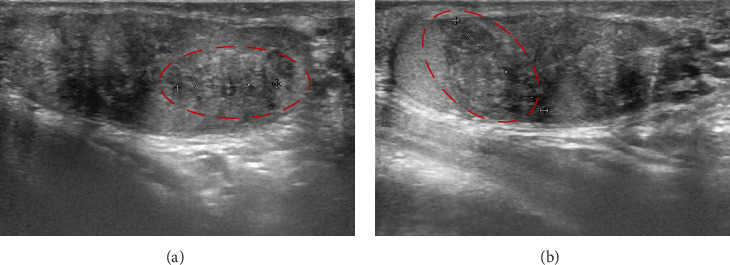
Congenital adrenal hyperplasia (CAH) due to 11-beta-hydroxylase deficiency (11-OHD) is the second most common steroidogenesis impairment in European populations, characterized by hypertension, hypokalemia, infertility, hyperandrogenism, and genital ambiguity in females. We present the case of a biological male patient with 11-OHD CAH who developed resistant hypertension, along with massive adrenal enlargement and testicular adrenal rests due to inadequate disease control while on dexamethasone treatment, compounded by drug interactions with his antiepileptic therapy. As the patient was reluctant to switch to a three-times-daily hydrocortisone regimen, he was transitioned to dual-release hydrocortisone, resulting in progressive improvement of most of his symptoms. This case highlights the importance of tailored therapy, particularly in rare diseases.
由于11-β-羟化酶缺乏(11-OHD)导致的先天性肾上腺增生(CAH)是欧洲人群中第二常见的类固醇生成障碍,其特征为高血压、低钾血症、不孕、高雄激素血症以及女性生殖器模糊。我们报告了一例患有11-OHD CAH的生物学男性患者,该患者在接受地塞米松治疗期间,由于疾病控制不佳,出现了顽固性高血压,同时伴有肾上腺肿大和睾丸肾上腺残余物,并且与他的抗癫痫治疗存在药物相互作用。由于患者不愿改用每日三次的氢化可的松治疗方案,因此将他转换为缓释氢化可的松治疗,其大多数症状逐渐得到改善。该病例突出了个体化治疗的重要性,尤其是在罕见病中。