Ke Yingjie, Hua Linbin, Pang Shanwen, Wang Qiuji, Zhong Lishan, Wang Zhenzhong, Zhou Kan, Zeng Rong, Huang Huanlei
Department of Cardiovascular Surgery, Guangdong Provincial People's Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, Guangdong, China.
Department of Cardiovascular Surgery, Guangdong Provincial People's Hospital's Nanhai Hospital, The Second People's Hospital of Nanhai District Foshan City, Foshan, Guangdong, China.
Front Surg. 2025 Apr 8;12:1532945. doi: 10.3389/fsurg.2025.1532945. eCollection 2025.
Tricuspid valve replacement (TVR), although accounting for a minority of heart valve surgeries, poses significant challenges, including poor patients' condition, prosthetic complications, and increased perioperative mortality rates. Despite preferences for valvuloplasty, some cases necessitate replacement. The choice of tricuspid valve type remains controversial, and there is no consensus on surgical risk factors. Additionally, long-term follow-up reports on a large number of cases are lacking. In this study, we aimed to analyze the medical records of the largest number of patients who underwent TVR surgery.
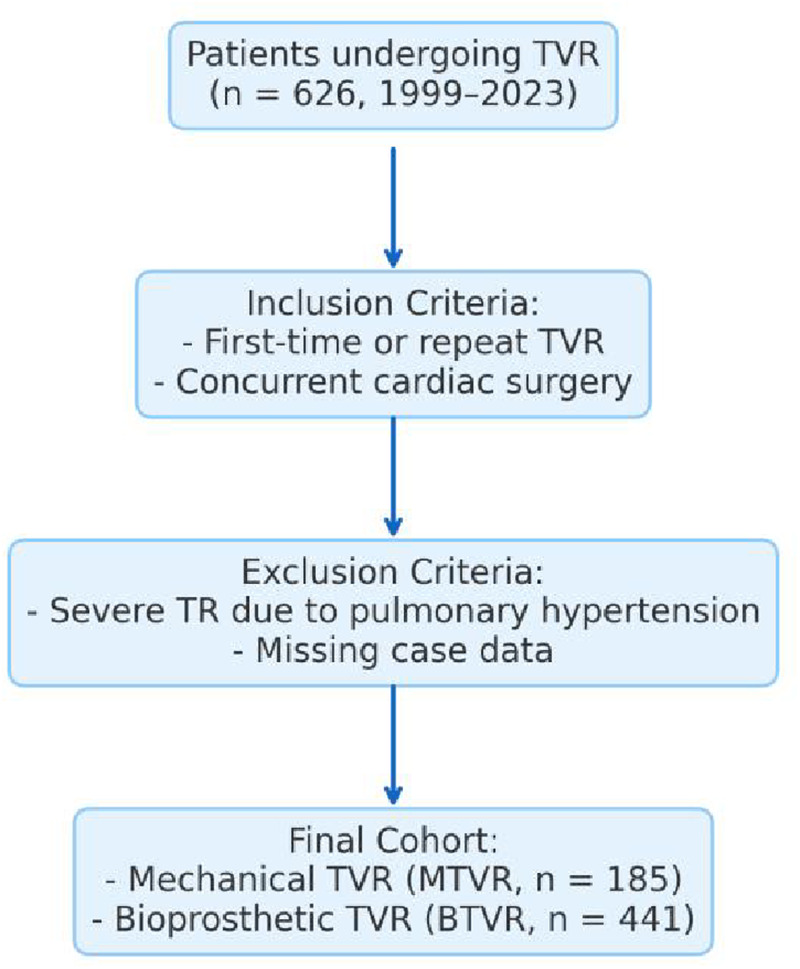
Patients who underwent TVR between 1999 and 2023 were divided into mechanical (MTVR) and bioprosthetic (BTVR) groups. Risk factors for overall mortality were analyzed.
In total, 626 patients were enrolled. The in-hospital and overall mortality rates were 12.1% and 42.8%, respectively. The in-hospital mortality rate (7.0% vs. 14.2%), incidence of acute renal insufficiency (4.3% vs. 12.2%), and hemodialysis rate (3.2% vs. 10.4%) were significantly higher in the BTVR group than in the MTVR group ( < 0.01). The median follow-up was 11 years (range 0.1-24 years). The MTVR group had significantly higher rates of long-term survival, hemorrhagic events, heart failure events, and re-operation rates than the BTVR group ( < 0.01). Multifactorial logistic regression analysis identified body weight, New York heart function classification, extracorporeal circulation time, and ventilator time as independent risk factors for in-hospital mortality. New York heart function classification during follow-up was identified as an independent risk factor for overall patient mortality.
MTVR was superior to BTVR regarding short- and long-term outcomes. New York heart function classification was associated with short- and long-term mortality.
三尖瓣置换术(TVR)虽然在心脏瓣膜手术中占少数,但带来了重大挑战,包括患者病情较差、人工瓣膜并发症以及围手术期死亡率增加。尽管人们更倾向于瓣膜成形术,但某些病例仍需要进行置换。三尖瓣类型的选择仍存在争议,对于手术风险因素也没有共识。此外,缺乏大量病例的长期随访报告。在本研究中,我们旨在分析接受TVR手术的患者数量最多的病历。
将1999年至2023年间接受TVR的患者分为机械瓣膜组(MTVR)和生物瓣膜组(BTVR)。分析总体死亡率的风险因素。
共纳入626例患者。住院死亡率和总体死亡率分别为12.1%和42.8%。BTVR组的住院死亡率(7.0%对14.2%)、急性肾功能不全发生率(4.3%对12.2%)和血液透析率(3.2%对10.4%)显著高于MTVR组(<0.01)。中位随访时间为11年(范围0.1 - 24年)。MTVR组的长期生存率、出血事件、心力衰竭事件和再次手术率显著高于BTVR组(<0.01)。多因素逻辑回归分析确定体重、纽约心脏功能分级、体外循环时间和呼吸机使用时间为住院死亡率的独立风险因素。随访期间的纽约心脏功能分级被确定为患者总体死亡率的独立风险因素。
在短期和长期结果方面,MTVR优于BTVR。纽约心脏功能分级与短期和长期死亡率相关。