Fischer Oliver Wedel, Justesen Tobias Freyberg, Gögenur Dilara Seyma, Madsen Michael Tvilling, Mortensen Michael Bau, Gögenur Ismail, Orhan Adile
Center for Surgical Science, Department of Surgery, Zealand University Hospital, 4600 Køge, Denmark.
Department of Surgery, Slagelse Sygehus, 4200 Slagelse, Denmark.
Cancers (Basel). 2025 Apr 14;17(8):1313. doi: 10.3390/cancers17081313.
Granulocyte-colony stimulating factor (G-CSF) prophylaxis is widely used in gastrointestinal (GI) cancers. The use of G-CSF in GI cancers has not previously been investigated systematically in a meta-analysis. Thus, we systematically reviewed the literature to describe the G-CSF use and potential influence on long-term oncological outcomes in GI cancers.
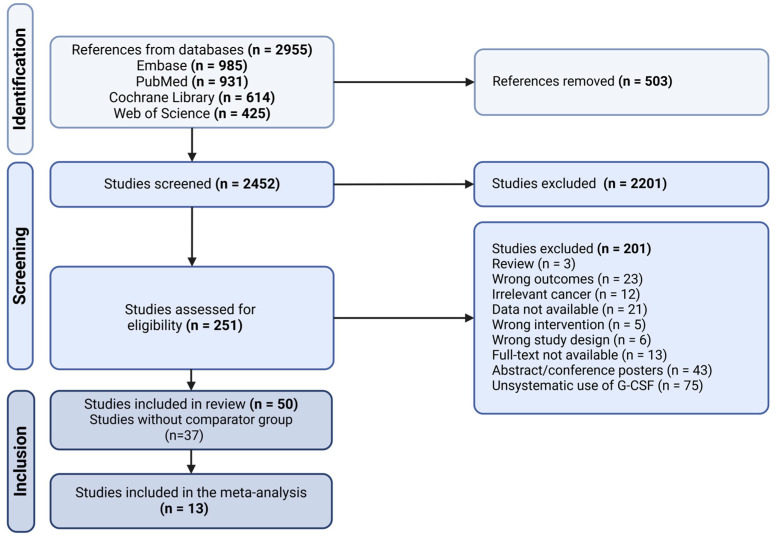
The literature search of this systematic review and meta-analysis was conducted in PubMed, Embase, Cochrane Library and Web of Science. The PRISMA-P guidelines were followed. Studies that reported data on patients with GI cancers undergoing oncological treatment with G-CSF prophylaxis were included. Outcomes of interest were overall survival (OS), progression-free survival (PFS) and adverse events (AE), specifically neutropenia grade III/IV. A time-to-event random-effects meta-analysis was conducted. Risk of bias was assessed using the Newcastle-Ottawa Scale and the Cochrane Risk of Bias Tool for Randomized Controlled Trials (RoB) tool.
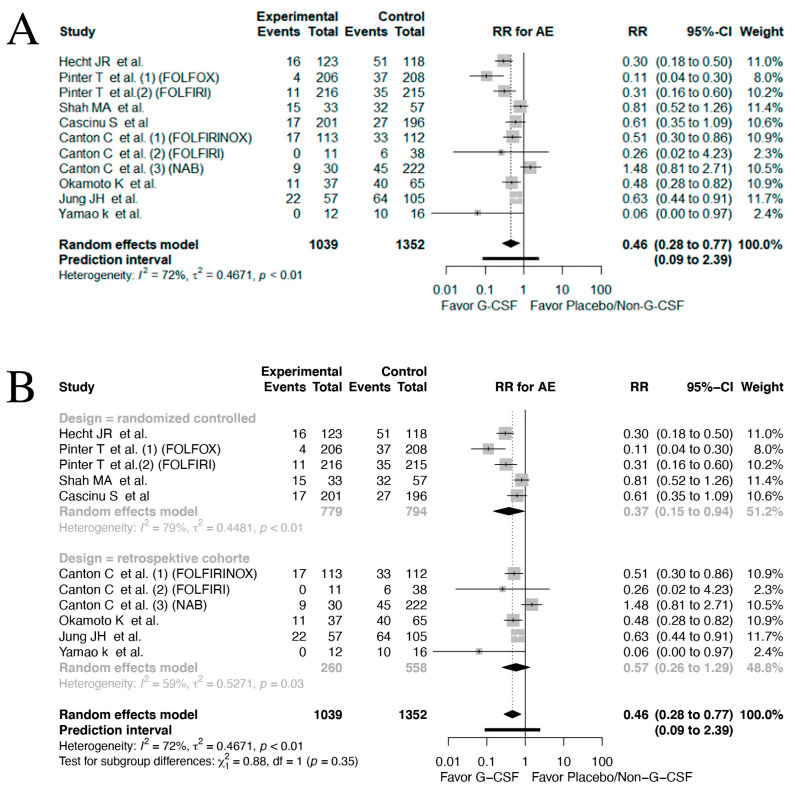
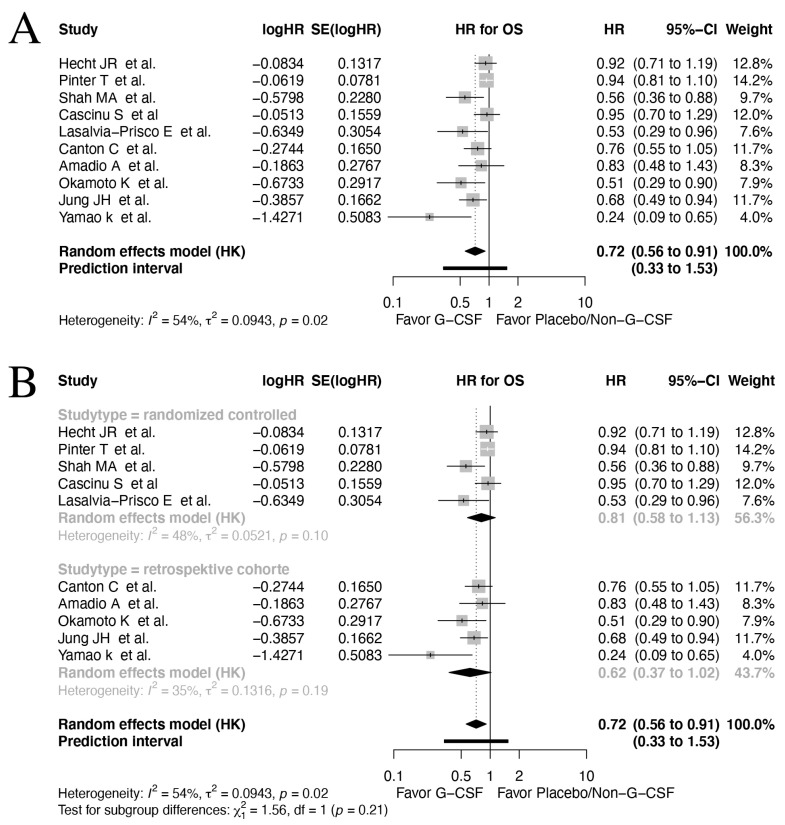
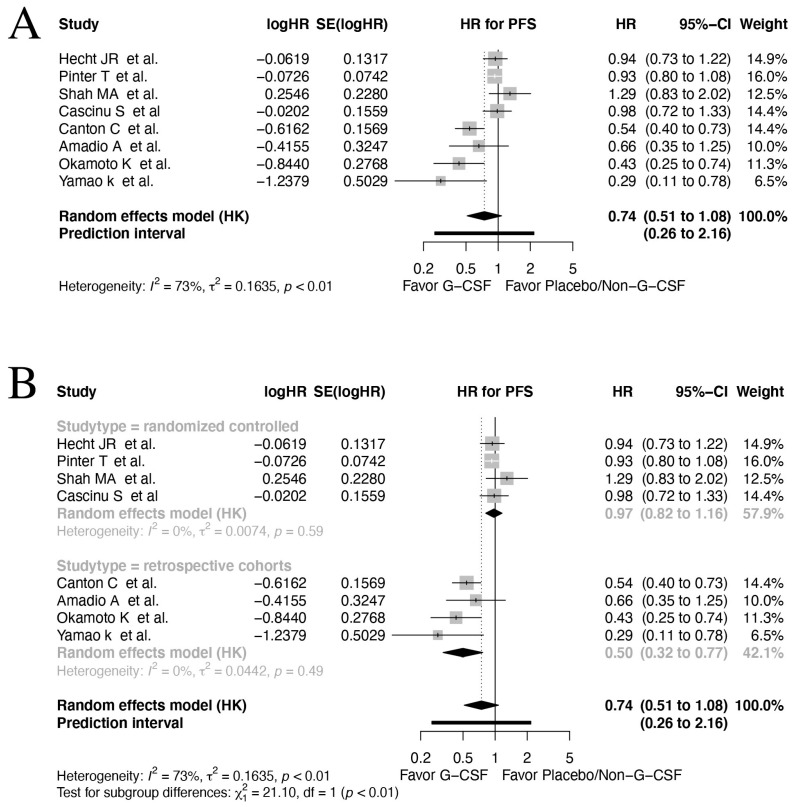
In total, 2452 articles were screened for eligibility. Ultimately, 13 studies were included with a total patient number of 2673. The included studies indicated a positive association between OS and G-CSF prophylaxis (HR 0.72, 95% CI: 0.56-0.91, : 54%, low quality evidence). No significant relation between G-CSF use and PFS was found in the pooled analyses (HR 0.74, 95% CI: 0.51-1.08, : 73%, moderate quality evidence). However, a positive effect of G-CSF use was found in the retrospective cohorts reporting data on PFS (HR 0.50, 95% CI: 0.32-0.77, : 0%). A marked drop in neutropenia grade III/IV rates was observed in patients treated with G-CSF (risk ratio (RR) 0.46, 95% CI: 0.28-0.77, : 72%, high quality evidence).
G-CSF prophylaxis provides a reduction in neutropenia grade III/IV in patients with GI cancers (high level of certainty) and a favorable OS (low certainty), while PFS is unaffected (moderate certainty). Studies on PFS and G-CSF use are nonetheless limited.
粒细胞集落刺激因子(G-CSF)预防措施在胃肠道(GI)癌症中被广泛应用。此前尚未通过荟萃分析对GI癌症中G-CSF的使用情况进行系统研究。因此,我们系统回顾了相关文献,以描述GI癌症中G-CSF的使用情况及其对长期肿瘤学结局的潜在影响。
本系统评价和荟萃分析的文献检索在PubMed、Embase、Cochrane图书馆和Web of Science中进行。遵循PRISMA-P指南。纳入报告接受G-CSF预防的肿瘤治疗的GI癌症患者数据的研究。感兴趣的结局包括总生存期(OS)、无进展生存期(PFS)和不良事件(AE),特别是III/IV级中性粒细胞减少。进行了事件时间随机效应荟萃分析。使用纽卡斯尔-渥太华量表和Cochrane随机对照试验偏倚风险工具(RoB)评估偏倚风险。
总共筛选了2452篇文章以确定其是否符合条件。最终,纳入了13项研究,患者总数为2673例。纳入的研究表明OS与G-CSF预防之间存在正相关(风险比[HR]0.72,95%置信区间[CI]:0.56 - 0.91,I²:54%,低质量证据)。在汇总分析中未发现G-CSF使用与PFS之间存在显著关系(HR 0.74,95% CI:0.51 - 1.08,I²:73%,中等质量证据)。然而,在报告PFS数据的回顾性队列中发现G-CSF使用有积极作用(HR 0.50,95% CI:0.32 - 0.77,I²:0%)。在接受G-CSF治疗的患者中观察到III/IV级中性粒细胞减少率显著下降(风险比[RR]0.46,95% CI:0.28 - 0.77,I²:72%,高质量证据)。
G-CSF预防可降低GI癌症患者的III/IV级中性粒细胞减少(高确定性),并改善OS(低确定性),而PFS不受影响(中等确定性)。然而,关于PFS和G-CSF使用的研究仍然有限。