Sanmartín-Sánchez Alicia, Fernández-Jiménez Rocío, Cabrera-César Eva, Espíldora-Hernández Francisco, Vegas-Aguilar Isabel, Amaya-Campos María Del Mar, Palmas-Candia Fiorella Ximena, Olivares-Alcolea Josefina, Simón-Frapolli Víctor José, Cornejo-Pareja Isabel, Sánchez-García Ana, Murri Mora, Guirado-Peláez Patricia, Vidal-Suárez Álvaro, Garrido-Sánchez Lourdes, Tinahones Francisco J, Velasco-Garrido Jose Luis, García-Almeida Jose Manuel
Department of Endocrinology and Nutrition, Son Espases University Hospital, 07120 Mallorca, Spain.
Department of Endocrinology and Nutrition, Virgen de la Victoria University Hospital, 29010 Malaga, Spain.
Life (Basel). 2025 Mar 21;15(4):516. doi: 10.3390/life15040516.
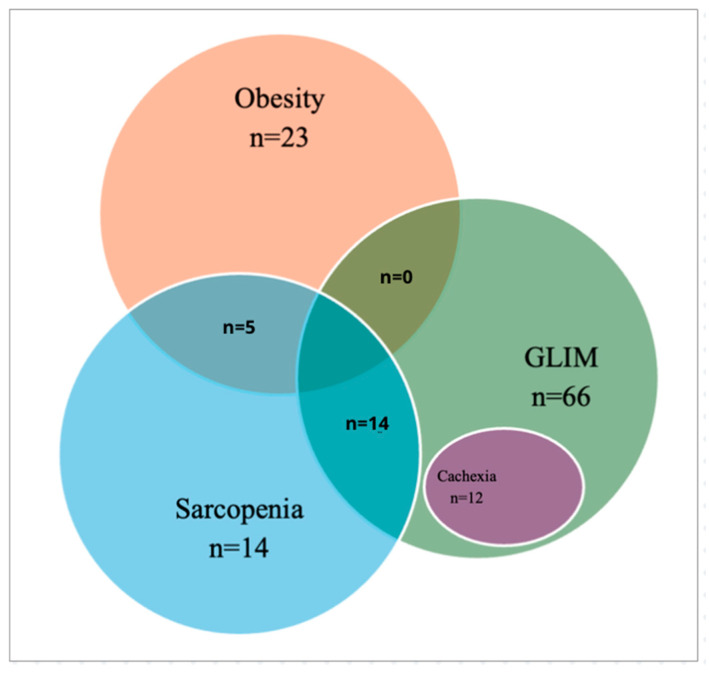
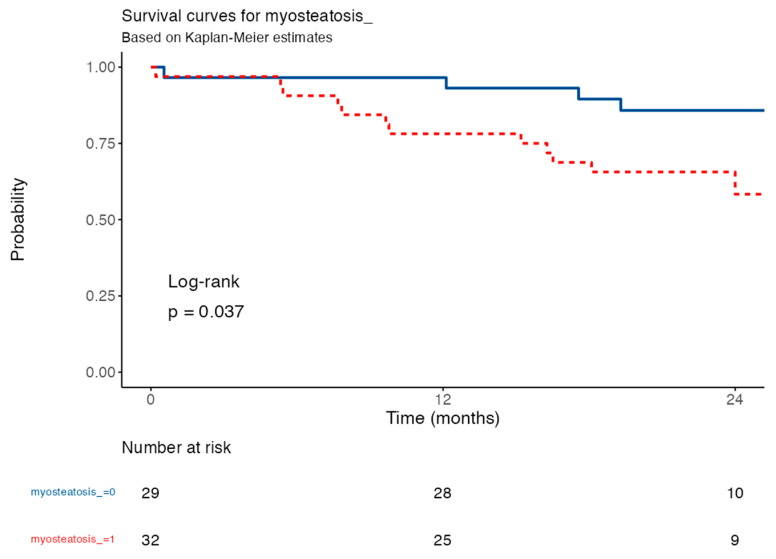
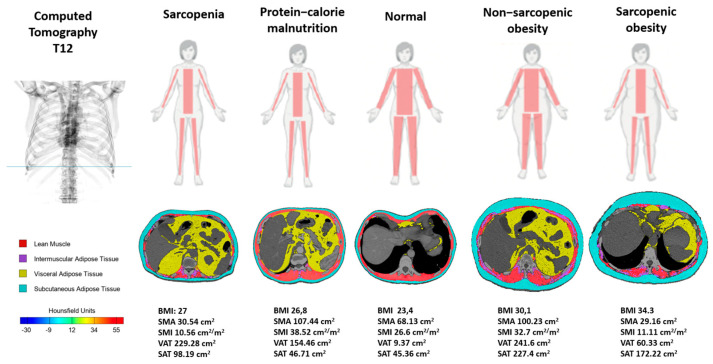
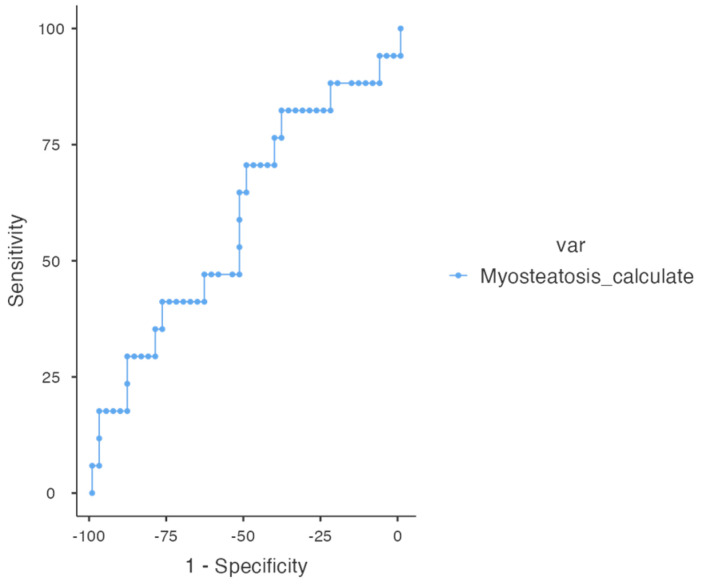
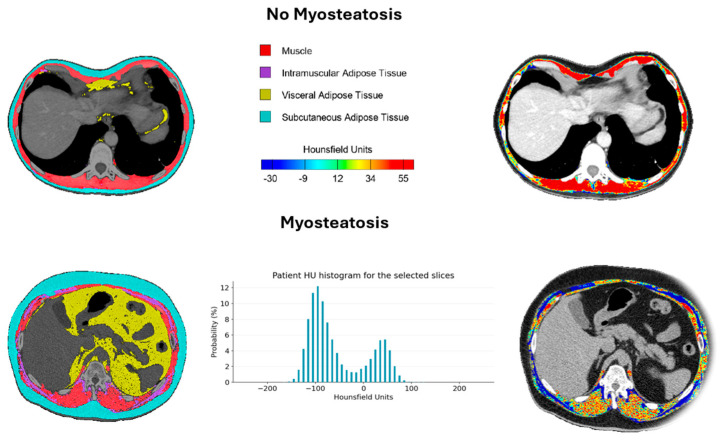
There is increasing evidence supporting the use of morphofunctional assessment (MFA) as a tool for clinical characterization and decision-making in malnourished patients. MFA enables the diagnosis of malnutrition, sarcopenia, obesity, and cachexia, leading to a novel phenotype-based classification of nutritional disorders. Bioelectrical impedance analysis (BIVA), nutritional ultrasound (NU) and computed tomography (CT) are included, along with functional tests like the Timed Up and Go test (TUG). Myoesteatosis, detectable via CT, can occur independently from nutritional phenotypes and has been identified as a significant mortality predictor in idiophatic pulmonary fibrosis (IPF). Our aim is to analyze the prevalence and overlap of nutritional phenotypes in IPF and evaluate the prognostic value of myoesteatosis. Our bicenter cross-sectional study included 82 IPF patients (84.1% male and with a medium age of 71.1 ± 7.35 years). MFA was performed using BIVA, NU, CT at the T12 level (CT-T12), the handgrip strength (HGS) test, and the TUG. CT-T12 BC parameters were analyzed using FocusedON software, while statistical analyses were conducted with JAMOVI version 2.3.22. All four major nutritional phenotypes were represented in our cohort, with significant overlap. A total of 80.5% met the GLIM criteria for malnutrition, 14.6% had cachexia, 17% were sarcopenic, and 28% were obese. Of the obese patients, 70% were also malnourished, while 100% of sarcopenic obese patients (5.9% of total) had malnutrition. A total of 55% of sarcopenic patients with available CT also had myosteatosis, suggesting muscle quality deterioration as a potential driver of functional impairment. The presence of myosteatosis > 15% in T12-CT was an independent predictor of 12-month mortality (HR = 3.13; 95% CI: 1.01-9.70; = 0.049), with survival rates of 78.1% vs. 96.6% in patients with vs. without myosteatosis, respectively. To conclude, this study underscores the relevance of MFA in the nutritional characterization of patients with IPF, demonstrating its potential to identify specific phenotypes associated with malnutrition, functional impairment, and the presence of thereby providing a valuable tool for clinical decision-making.
越来越多的证据支持使用形态功能评估(MFA)作为营养不良患者临床特征描述和决策的工具。MFA能够诊断营养不良、肌肉减少症、肥胖症和恶病质,从而形成一种基于新表型的营养障碍分类。生物电阻抗分析(BIVA)、营养超声(NU)和计算机断层扫描(CT)都被纳入其中,还有诸如计时起立行走测试(TUG)等功能测试。通过CT可检测到的肌脂肪变性可独立于营养表型出现,并且已被确定为特发性肺纤维化(IPF)的一个重要死亡预测指标。我们的目的是分析IPF中营养表型的患病率和重叠情况,并评估肌脂肪变性的预后价值。我们的双中心横断面研究纳入了82例IPF患者(84.1%为男性,平均年龄为71.1±7.35岁)。使用BIVA、NU、T12水平的CT(CT-T12)、握力(HGS)测试和TUG进行MFA。使用FocusedON软件分析CT-T12的BC参数,同时使用JAMOVI 2.3.22版本进行统计分析。我们的队列中所有四种主要营养表型均有体现,且有显著重叠。共有80.5%的患者符合营养不良的GLIM标准,14.6%的患者患有恶病质,17%的患者有肌肉减少症,28%的患者肥胖。在肥胖患者中,70%也存在营养不良,而所有肌肉减少性肥胖患者(占总数的5.9%)均有营养不良。在有可用CT的肌肉减少症患者中,共有55%也存在肌脂肪变性,这表明肌肉质量下降可能是功能障碍的一个潜在驱动因素。T12-CT中肌脂肪变性>15%的存在是12个月死亡率的独立预测指标(HR = 3.13;95% CI:1.01 - 9.70;P = 0.049),有肌脂肪变性的患者与无肌脂肪变性的患者的生存率分别为78.1%和96.6%。总之,本研究强调了MFA在IPF患者营养特征描述中的相关性,证明了其识别与营养不良、功能障碍相关的特定表型以及肌脂肪变性存在的潜力,从而为临床决策提供了一个有价值的工具。