Barbosa Galindo Vinicius, Midega Thais Dias, Souza Guilherme Martins de, Hohmann Fábio Barlem, Assis Mayara Laise, Cordioli Ricardo Luiz, Rodrigues Roseny Dos Reis, de Matos Gustavo Faissol Janot, Pardini Andréia, Jaures Michele, de Arruda Bravim Bruno, Laselva Claudia Regina, Fernandes Constantino Jose, Corrêa Thiago Domingos
Intensive Care Unit - Hospital Israelita Albert Einstein, São Paulo, Brazil.
PLoS One. 2025 Apr 28;20(4):e0317429. doi: 10.1371/journal.pone.0317429. eCollection 2025.
It has been demonstrated that the implementation of rapid response teams (RRT) may improve clinical outcomes. Nevertheless, predictors of mortality among patients admitted to the intensive care unit (ICU) or to the step-down unit (SDU) after a RRT activation are not fully understood.
To describe clinical characteristics, resource use, main outcomes, and to address predictors of in-hospital mortality among patients admitted to the ICU/SDU after RRT activation.
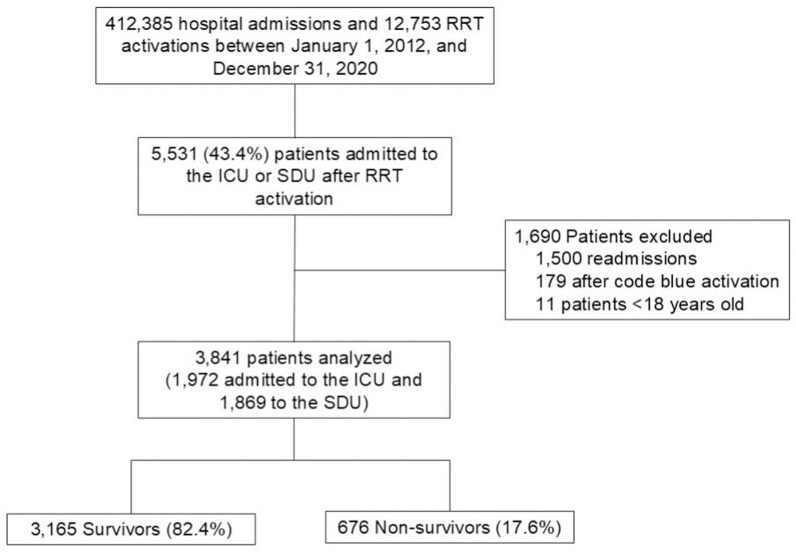
Retrospective single-center cohort study conducted in a medical-surgical ICU/SDU located in a private quaternary care hospital. Adult patients admitted to the ICU or SDU between 2012 and 2020 were compared according to in-hospital mortality. A multivariate logistic regression analysis was performed to identify independent predictors of in-hospital mortality.
Among the 3841 patients included in this analysis [3165 (82.4%) survivors and 676 (17.6%) non-survivors], 1972 (51.3%) were admitted to the ICU and 1869 (48.7%) were admitted to the SDU. Compared to survivors, non-survivors were older [76 (64-87) yrs. vs. 67 (50-81) yrs.; p < 0.001], had a higher SAPS 3 score [64 (56-72) vs. 49 (40-57); p < 0.001], and had a longer length of stay (LOS) before unit admission [8 (3-19) days vs. 2 (1-7) days; p < 0.001). Non-survivors used more non-invasive ventilation (NIV) (42.2% vs. 20.9%; p < 0.001), mechanical ventilation (MV) (36.7% vs. 9.3%; p < 0.001), vasopressors (39.2% vs. 12.3%; p < 0.001), renal replacement therapy (15.5% vs. 4.3%; p < 0.001), and blood components transfusion (34.9% vs. 14.0%; p < 0.001). Independent predictors of in-hospital mortality were the SAPS 3 score, the Charlson Comorbidity Index, LOS before unit admission, immunosuppression, respiratory rate < 8 or > 28 ipm criteria for RRT activation, RRT activation during the night shift, and the need for high-flow nasal cannula, NIV, MV, vasopressors, and blood components transfusion.
Multiple factors may affect outcomes of ICU/SDU-admitted patients after RRT activation. Therefore, efforts should be made to boost RRT effectiveness to improve patient safety.
已有研究表明,快速反应团队(RRT)的实施可能改善临床结局。然而,RRT启动后入住重症监护病房(ICU)或降级病房(SDU)的患者死亡率的预测因素尚未完全明确。
描述RRT启动后入住ICU/SDU患者的临床特征、资源利用情况、主要结局,并探讨院内死亡的预测因素。
在一家私立四级护理医院的内科/外科ICU/SDU进行回顾性单中心队列研究。根据院内死亡率对2012年至2020年间入住ICU或SDU的成年患者进行比较。进行多因素逻辑回归分析以确定院内死亡的独立预测因素。
在本分析纳入的3841例患者中[3165例(82.4%)存活,676例(17.6%)未存活],1972例(51.3%)入住ICU,1869例(48.7%)入住SDU。与存活患者相比,未存活患者年龄更大[76(64 - 87)岁 vs. 67(50 - 81)岁;p < 0.001],急性生理与慢性健康状况评分系统(SAPS)3评分更高[64(56 - 72) vs. 49(40 - 57);p < 0.001],入院前住院时间更长[8(3 - 19)天 vs. 2(1 - 7)天;p < 0.001]。未存活患者使用更多无创通气(NIV)(42.2% vs. 20.9%;p < 0.001)、机械通气(MV)(36.7% vs. 9.3%;p < 0.001)、血管活性药物(39.2% vs. 12.3%;p < 0.001)、肾脏替代治疗(15.5% vs. 4.3%;p < 0.001)和血液成分输血(34.9% vs. 14.0%;p < 0.001)。院内死亡的独立预测因素包括SAPS 3评分、Charlson合并症指数、入院前住院时间、免疫抑制、RRT启动的呼吸频率<8次/分钟或>28次/分钟标准、夜班期间RRT启动以及对高流量鼻导管、NIV、MV、血管活性药物和血液成分输血的需求。
RRT启动后,多种因素可能影响入住ICU/SDU患者的结局。因此,应努力提高RRT的有效性以改善患者安全。