Kritz Erin M, Thomas Jenilea K, Alawa Nawara S, Hadad Elit B, Guffey Danielle M, Bavare Aarti C
Department of Pediatric Critical Care, Baylor College of Medicine, Houston, TX, United States.
Department of Pediatrics, Texas Children's Hospital, Houston, TX, United States.
Front Pediatr. 2023 Jun 14;11:1208873. doi: 10.3389/fped.2023.1208873. eCollection 2023.
We describe the characteristics and outcomes of pediatric rapid response team (RRT) events within a single institution, categorized by reason for RRT activation (RRT triggers). We hypothesized that events with multiple triggers are associated with worse outcomes.
Retrospective 3-year study at a high-volume tertiary academic pediatric hospital. We included all patients with index RRT events during the study period.
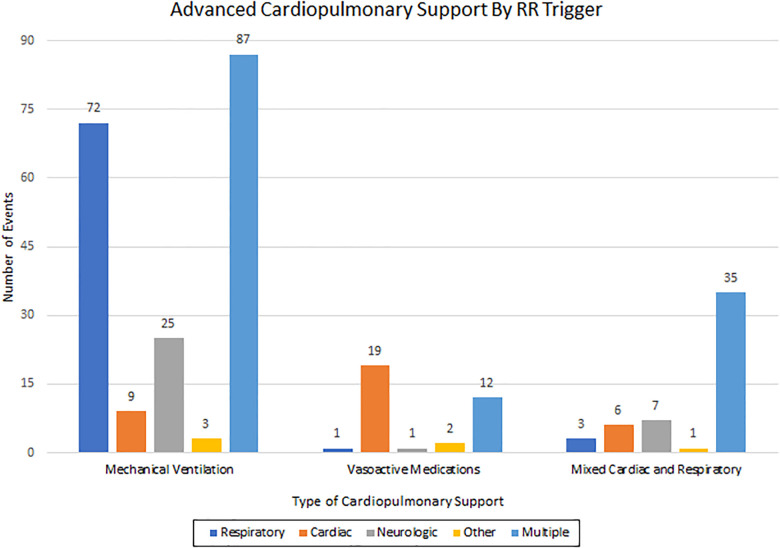
Association of patient and RRT event characteristics with outcomes including transfers to ICU, need for advanced cardiopulmonary support, ICU and hospital length of stay (LOS), and mortality were studied. We reviewed 2,267 RRT events from 2,088 patients. Most (59%) were males with a median age of 2 years and 57% had complex chronic conditions. RRT triggers were: respiratory (36%) and multiple (35%). Transfer to the ICU occurred after 1,468 events (70%). Median hospital and ICU LOS were 11 and 1 days. Need for advanced cardiopulmonary support was noted in 291 events (14%). Overall mortality was 85 (4.1%), with 61 (2.9%) of patients having cardiopulmonary arrest (CPA). Multiple RRT trigger events were associated with transfer to the ICU (559 events; OR 1.48; < 0.001), need for advanced cardiopulmonary support (134 events; OR 1.68; < 0.001), CPA (34 events; OR 2.36; = 0.001), and longer ICU LOS (2 vs. 1 days; < 0.001). All categories of triggers have lower odds of need for advanced cardiopulmonary support than multiple triggers (OR 1.73; < 0.001).
RRT events with multiple triggers were associated with cardiopulmonary arrest, transfer to ICU, need for cardiopulmonary support, and longer ICU LOS. Knowledge of these associations can guide clinical decisions, care planning, and resource allocation.
我们描述了单一机构内儿科快速反应团队(RRT)事件的特征和结果,并根据RRT启动原因(RRT触发因素)进行分类。我们假设具有多个触发因素的事件与更差的结果相关。
在一家大型三级学术儿科医院进行的为期3年的回顾性研究。我们纳入了研究期间所有首次发生RRT事件的患者。
研究了患者和RRT事件特征与结果之间的关联,这些结果包括转入重症监护病房(ICU)、需要高级心肺支持、ICU和医院住院时间(LOS)以及死亡率。我们回顾了来自2088名患者的2267次RRT事件。大多数(59%)为男性,中位年龄为2岁,57%患有复杂慢性病。RRT触发因素为:呼吸相关(36%)和多种因素(35%)。1468次事件(70%)后转入ICU。中位住院时间和ICU住院时间分别为11天和1天。291次事件(14%)中记录了需要高级心肺支持。总体死亡率为85例(4.1%),其中61例(2.9%)患者发生心肺骤停(CPA)。多个RRT触发因素事件与转入ICU(559次事件;比值比[OR]1.48;P<0.001)、需要高级心肺支持('134次事件;OR 1.68;P<0.001)、CPA(34次事件;OR 2.36;P=0.001)以及更长的ICU住院时间(2天对1天;P<0.001)相关。所有类别的触发因素比多个触发因素需要高级心肺支持的几率更低(OR 1.73;P<0.001)。
具有多个触发因素的RRT事件与心肺骤停、转入ICU、需要心肺支持以及更长的ICU住院时间相关。了解这些关联可为临床决策、护理计划和资源分配提供指导。