Acharya Dilaram, Scory Tayler D, Shommu Nusrat, Donald Maoliosa, Harrison Tyrone G, Murray Jonathan S, Sawhney Simon, Siew Edward D, Pannu Neesh, James Matthew T
Department of Medicine, Cumming School of Medicine, University of Calgary, AB, Canada.
Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, AB, Canada.
Can J Kidney Health Dis. 2025 Apr 30;12:20543581251336548. doi: 10.1177/20543581251336548. eCollection 2025.
Patients hospitalized with acute kidney injury (AKI) have variable risks for chronic kidney disease (CKD); however, there is limited knowledge about how this risk influences outpatient follow-up with nephrologists.
This survey study examined the likelihood that nephrologists would recommend outpatient follow-up of patients with varying risk profiles for CKD after hospitalization with AKI and the effect of reporting the predicted risk of severe CKD on their decision-making.
A randomized survey study examining the impact of providing predicted risks of severe CKD on nephrologists' follow-up recommendations for patients with AKI.
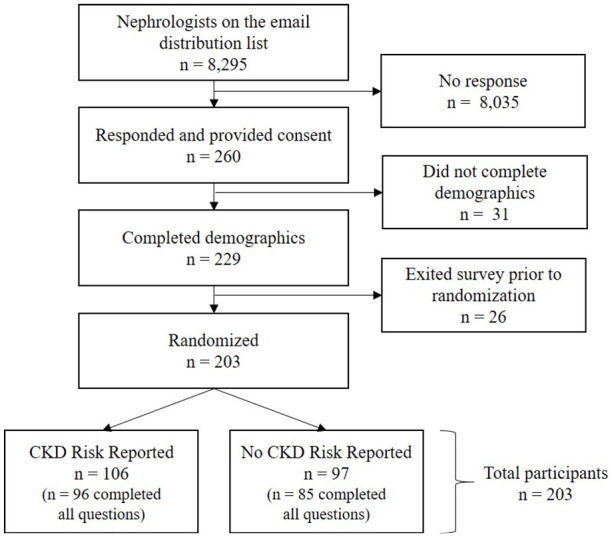
The study included nephrologists from the United States, the United Kingdom, and Canada between September and December 2023.
Participants reviewed clinical vignettes of patients with AKI and varying risks of severe CKD (G4 or G5), using an externally validated prediction model.
The primary outcome was the likelihood of recommending nephrologist specialist follow-up for each case, scored on a 7-point Likert scale (1 = "definitely not" and 7 = "definitely would").
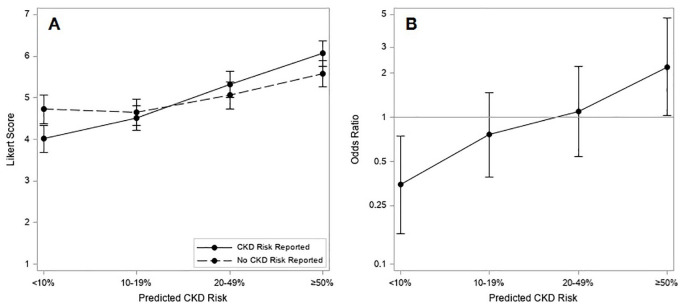
Participants were randomized to receive a version of the survey either with or without the predicted risk of severe CKD included for each vignette. Responses were compared across categories of predicted risk (<10%, 10%-49%, and ≥50%) using generalized estimating equations.
Of the 203 nephrologists who participated, 73 (36%) were from the United Kingdom, 71 (35%) from Canada, and 45 (22%) from the United States. Mean (95% confidence interval [CI]) Likert scores increased from 4.01 (3.68, 4.34) for patients with a <10% predicted risk to 6.06 (5.76, 6.37) for those with a ≥ 50% predicted risk of severe CKD. Nephrologists were significantly less likely to recommend outpatient nephrology follow-up for patients with a <10% predicted risk of severe CKD when the risk was reported (mean difference = -0.71 [95% CI = -1.19, -0.23]), and significantly more likely to recommend follow-up for patients with a ≥50% predicted risk when the risk of severe CKD was reported (mean difference = 0.49 [95% CI = 0.04, 0.93]).
This study focuses on nephrologists from high-income countries and relies on hypothetical scenarios rather than real-world practices. Survey respondents may not be representative of all nephrologists, although consistent findings across diverse subgroups strengthen findings.
When the predicted risk of severe CKD is reported, nephrologists are less likely to recommend follow-up for lower risk patients with AKI and more likely to recommend follow-up for higher risk patients, leading to better alignment of recommendations for outpatient follow-up with patient risk of severe CKD.
急性肾损伤(AKI)住院患者患慢性肾脏病(CKD)的风险各不相同;然而,对于这种风险如何影响肾病科医生的门诊随访,人们了解有限。
这项调查研究探讨了肾病科医生对AKI住院后CKD风险不同的患者进行门诊随访的可能性,以及报告严重CKD预测风险对其决策的影响。
一项随机调查研究,考察提供严重CKD预测风险对肾病科医生对AKI患者随访建议的影响。
该研究纳入了2023年9月至12月期间来自美国、英国和加拿大的肾病科医生。
参与者使用经过外部验证的预测模型,回顾了AKI患者以及严重CKD(G4或G5)不同风险的临床病例。
主要结果是对每个病例推荐肾病科专科随访的可能性,采用7分李克特量表评分(1 =“绝对不会”,7 =“肯定会”)。
参与者被随机分配接受包含或不包含每个病例严重CKD预测风险的调查问卷版本。使用广义估计方程对预测风险类别(<10%、10%-49%和≥50%)的回答进行比较。
参与的203名肾病科医生中,73名(36%)来自英国,71名(35%)来自加拿大,45名(22%)来自美国。李克特平均评分(95%置信区间[CI])从预测风险<10%的患者的4.01(3.68,4.34)增加到严重CKD预测风险≥50%的患者的6.06(5.76,6.37)。当报告风险时,肾病科医生对严重CKD预测风险<10%的患者推荐门诊肾病随访的可能性显著降低(平均差异=-0.71[95%CI=-1.19,-0.23]),而当报告严重CKD风险时,对预测风险≥50%的患者推荐随访更为可能(平均差异=0.49[95%CI=0.04,0.93])。
本研究聚焦于高收入国家的肾病科医生,且依赖假设情景而非实际临床实践。调查受访者可能无法代表所有肾病科医生,尽管不同亚组的一致发现强化了研究结果。
当报告严重CKD的预测风险时,肾病科医生对低风险AKI患者推荐随访的可能性降低,对高风险患者推荐随访的可能性增加,从而使门诊随访建议与患者严重CKD风险更好地匹配。