Aberdeen Centre for Health Data Sciences, University of Aberdeen, Aberdeen, Scotland; National Health Service Grampian, Aberdeen, Scotland.
Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Am J Kidney Dis. 2021 Jul;78(1):28-37. doi: 10.1053/j.ajkd.2020.12.008. Epub 2021 Jan 9.
RATIONALE & OBJECTIVE: There is limited evidence to guide follow-up after acute kidney injury (AKI). Knowledge gaps include which patients to prioritize, at what time point, and for mitigation of which outcomes. In this study, we sought to compare the net benefit of risk model-based clinical decisions following AKI.
External validation of 2 risk models of AKI outcomes: the Grampian -Aberdeen (United Kingdom) AKI readmissions model and the Alberta (Canada) kidney disease risk model of chronic kidney disease (CKD) glomerular (G) filtration rate categories 4 and 5 (CKD G4 and G5). Process mining to delineate existing care pathways.
SETTING & PARTICIPANTS: Validation was based on data from adult hospital survivors of AKI from Grampian, 2011-2013.
KDIGO-based measures of AKI severity and comorbidities specified in the original models.
Death or readmission within 90 days for all hospital survivors. Progression to new CKD G4-G5 for patients surviving at least 90 days after AKI.
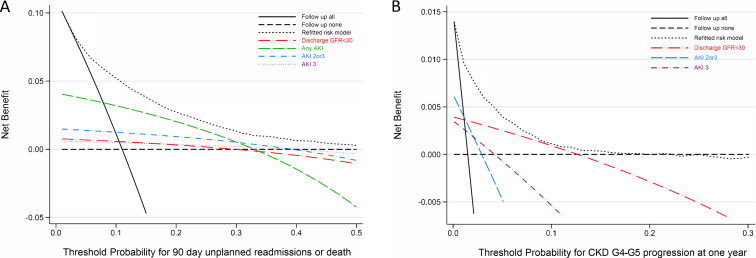
Decision curve analysis to assess the "net benefit" of use of risk models to guide clinical care compared to alternative approaches (eg, prioritizing all AKI, severe AKI, or only those without kidney recovery).
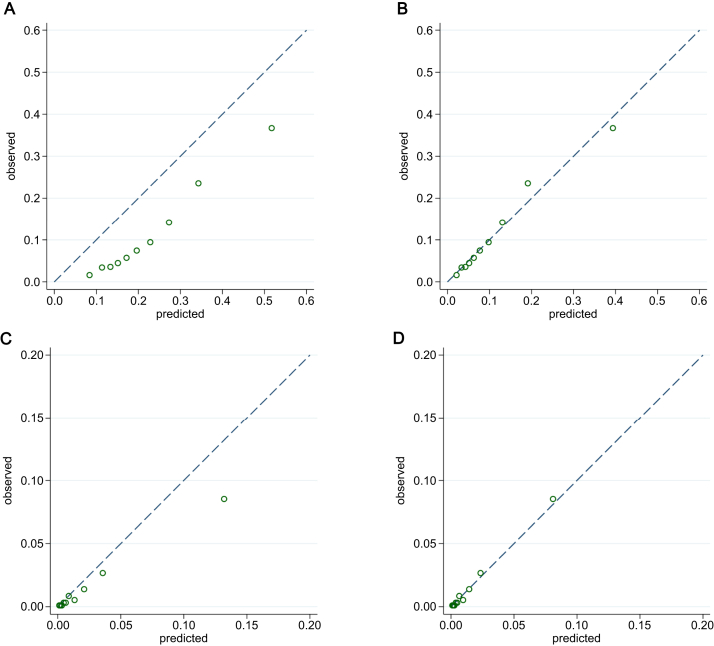
26,575 of 105,461 hospital survivors in Grampian (mean age, 60.9 ± 19.8 [SD] years) were included for validation of the death or readmission model, and 9,382 patients (mean age, 60.9 ± 19.8 years) for the CKD G4-G5 model. Both models discriminated well (area under the curve [AUC], 0.77 and 0.86, respectively). Decision curve analysis showed greater net benefit for follow up of all AKI than only severe AKI in most cases. Both original and refitted models provided net benefit superior to any other decision strategy. In process mining of all hospital discharges, 41% of readmissions and deaths occurred among people recovering after AKI. 1,464 of 3,776 people (39%) readmitted after AKI had received no intervening monitoring.
Both original models overstated risks, indicating a need for regular updating.
Follow up after AKI has potential net benefit for preempting readmissions, death, and subsequent CKD progression. Decisions could be improved by using risk models and by focusing on AKI across a full spectrum of severity. The current lack of monitoring among many with poor outcomes indicates possible opportunities for implementation of decision support.
急性肾损伤(AKI)后,指导随访的证据有限。知识空白包括应优先考虑哪些患者、在何时以及针对哪些结局进行缓解。本研究旨在比较 AKI 后基于风险模型的临床决策的净获益。
对 2 个 AKI 结局风险模型(英国 Grampian-Aberdeen AKI 再入院模型和加拿大阿尔伯塔肾脏疾病慢性肾脏病(CKD)肾小球(G)滤过率 4 和 5 类别风险模型(CKD G4 和 G5))进行外部验证。流程挖掘以描绘现有护理途径。
验证基于 Grampian 2011-2013 年 AKI 成年医院幸存者的数据。
KDIGO 定义的 AKI 严重程度和原始模型中指定的合并症。
所有医院幸存者 90 天内死亡或再入院。至少在 AKI 后 90 天存活的患者进展为新的 CKD G4-G5。
决策曲线分析,以评估与替代方法(例如,优先考虑所有 AKI、严重 AKI 或仅无肾脏恢复的患者)相比,使用风险模型指导临床护理的“净获益”。
Grampian 105461 例医院幸存者中的 26575 例(平均年龄 60.9±19.8[SD]岁)用于验证死亡或再入院模型,9382 例患者(平均年龄 60.9±19.8 岁)用于 CKD G4-G5 模型。两个模型均能很好地区分(曲线下面积[AUC],分别为 0.77 和 0.86)。决策曲线分析表明,在大多数情况下,与仅严重 AKI 相比,对所有 AKI 的随访具有更大的净获益。原始和重新拟合的模型均提供优于任何其他决策策略的净获益。在所有医院出院的流程挖掘中,41%的再入院和死亡发生在 AKI 后恢复的人群中。1464 名(39%)AKI 后再入院的患者未接受任何中间监测。
两个原始模型都过高估计了风险,表明需要定期更新。
AKI 后的随访可能对预防再入院、死亡和随后的 CKD 进展具有潜在的净获益。通过使用风险模型和关注 AKI 的全严重程度范围,可以改善决策。当前,许多预后不良的患者缺乏监测,这可能为实施决策支持提供机会。