Zhang Xiao-Qiang, Tang Run-Xi, Pan Dong-Hao, Zhang Chao-Fu, Xia Ming-Yang, Shuai Lei-Yuan, Tang Hua, Ji Guang-Yan
Department of Gastrointestinal Surgery, The First Affiliated Hospital of Chongqing Medical University, No. 1 Youyi Road, Yuanjiagang District, Chongqing, 400016, China.
Shanxi Provincial Institute of Traditional Chinese Medicine, Taiyuan, 030021, Shanxi, China.
Int J Colorectal Dis. 2025 May 5;40(1):109. doi: 10.1007/s00384-025-04897-8.
This study aims to compare laparoscopic versus open in ileostomy reversal techniques from multiple perspectives and to gain insight into the potential advantages and limitations of laparoscopic techniques and provide guidance on finding the best anastomosis for ileostomy reversal.
This systematic review and meta-analysis has been pre-registered with PROSPERO. The registration number is CRD42025640754. A rigorous literature search was conducted across multiple databases, including Embase, PubMed, Cochrane Library, and China National Knowledge Infrastructure. The primary outcome measure was the incidence of overall postoperative complications, and the secondary outcomes included operative time, estimated blood loss, and the length hospital stay.
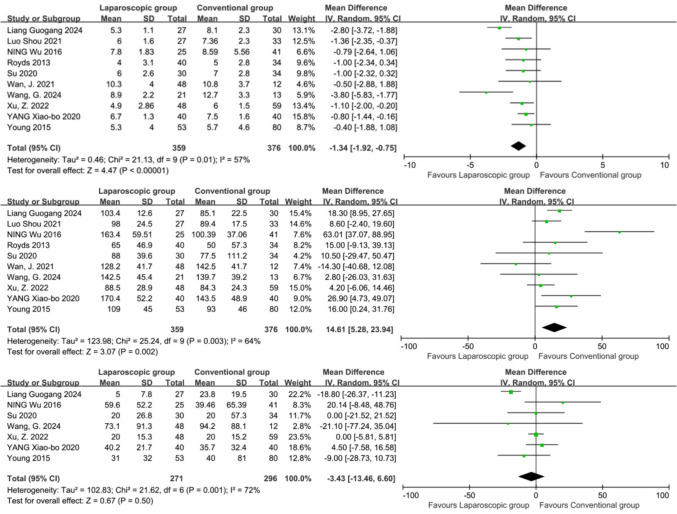
This research included 11 studies with a total of 867 cases, showing that the laparoscopic surgery group had a significantly lower overall complication rate compared to the open surgery group (OR = 0.40, 95% CI: 0.27-0.59, P < 0.00001). Further investigation of specific postoperative complications revealed that laparoscopic surgery significantly reduced the risk of bowel obstruction (OR = 0.39, 95% CI: 0.18-0.83, P = 0.01) and wound infection (OR = 0.41, 95% CI: 0.23-0.73, P = 0.003), with no significant difference observed for anastomotic leaks (OR = 0.40, 95% CI: 0.11-1.43, P = 0.16). Although laparoscopic surgery required a longer operative time (P = 0.002), it resulted in significantly shorter hospital stays (P < 0.00001) and did not increase estimated blood loss (P = 0.50). In addition, both extracorporeal laparoscopic surgery and intracorporeal laparoscopic surgery can effectively reduce the occurrence of postoperative complications and shorten the length of hospital stay compared with open surgery.
Laparoscopic-assisted ileostomy closure (both intracorporeal and extracorporeal techniques) demonstrates significant clinical benefits, including reduced postoperative complication rates, shortened hospitalization duration, and optimized recovery trajectories.
本研究旨在从多个角度比较腹腔镜与开放回肠造口术回纳技术,深入了解腹腔镜技术的潜在优势和局限性,并为寻找回肠造口术回纳的最佳吻合方式提供指导。
本系统评价和荟萃分析已在PROSPERO进行预注册。注册号为CRD42025640754。在多个数据库中进行了严格的文献检索,包括Embase、PubMed、Cochrane图书馆和中国知网。主要结局指标为术后总体并发症发生率,次要结局包括手术时间、估计失血量和住院时间。
本研究纳入11项研究,共867例病例,结果显示腹腔镜手术组的总体并发症发生率显著低于开放手术组(OR = 0.40,95%CI:0.27 - 0.59,P < 0.00001)。对特定术后并发症的进一步调查显示,腹腔镜手术显著降低了肠梗阻风险(OR = 0.39,95%CI:0.18 - 0.83,P = 0.01)和伤口感染风险(OR = 0.41,95%CI:0.23 - 0.73,P = 0.003),吻合口漏方面未观察到显著差异(OR = 0.40,95%CI:0.11 - 1.43,P = 0.16)。虽然腹腔镜手术需要更长的手术时间(P = 0.002),但住院时间显著缩短(P < 0.00001),且未增加估计失血量(P = 0.50)。此外,与开放手术相比,体外腹腔镜手术和体内腹腔镜手术均能有效降低术后并发症的发生并缩短住院时间。
腹腔镜辅助回肠造口关闭术(包括体内和体外技术)显示出显著的临床益处,包括降低术后并发症发生率、缩短住院时间和优化恢复过程。