Nguyen Nhan, Ho Quang Tri Vinh, Nguyen Ngoc Dan Vy, Bao Tran Nghi, Olah Laszlo, Heja Mate
Faculty of Medicine, University of Debrecen, Debrecen, Hungary.
Faculty of Medicine, University of Melbourne, Melbourne, Australia.
J Headache Pain. 2025 May 6;26(1):99. doi: 10.1186/s10194-025-02047-7.
The use of monoclonal antibodies targeting Calcitonin Gene-Related Peptide (CGRP) is an established treatment for chronic migraine (CM). However, its efficacy in CM patients with medication overuse headache (MOH) remains underexplored, and data on the safety and patient compliance of standard-to-high doses, especially Eptinezumab and Erenumab, over at least three months are limited.
This study aims to evaluate the efficacy and safety of anti-CGRP therapy (Eptinezumab and Erenumab) in CM and MOH patients. Specifically, it assesses changes in monthly migraine days (MMDs) after 12 weeks, risk of treatment-emergent adverse events (TEAEs) leading to discontinuation, serious TEAEs, common adverse effects, and MOH remission at 6 months.
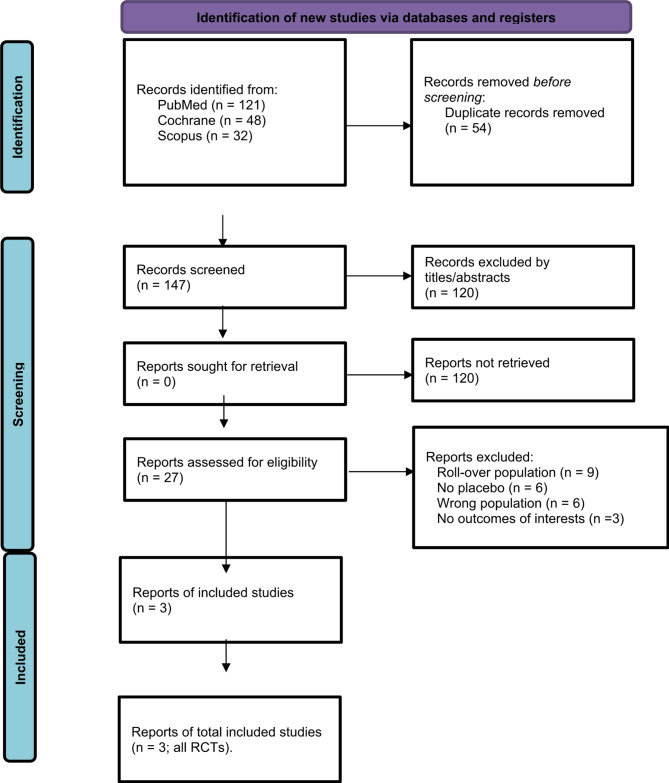
A systematic search of PubMed, Cochrane, and Scopus databases identified randomized controlled trials (RCTs) evaluating standard or high dose anti-CGRP therapy in CM patients strictly with MOH. Studies included were required to report a ≥ 50% reduction in MMDs after ≥ 12 weeks, serious TEAEs, TEAEs leading to discontinuation, common adverse events, and MOH remission at 6 months. Heterogeneity was assessed using I² statistics and a random-effects model.
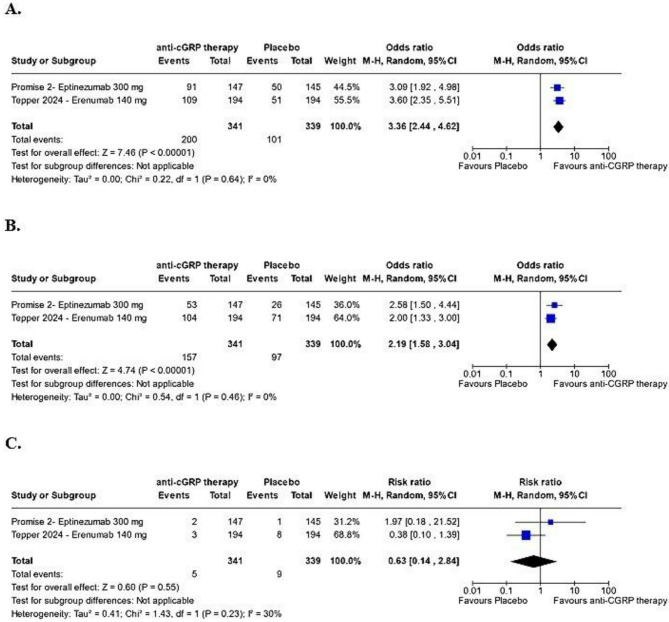
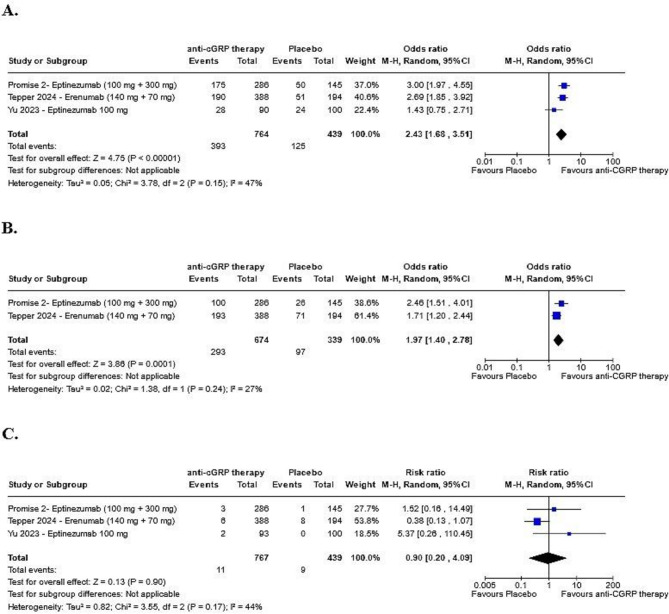
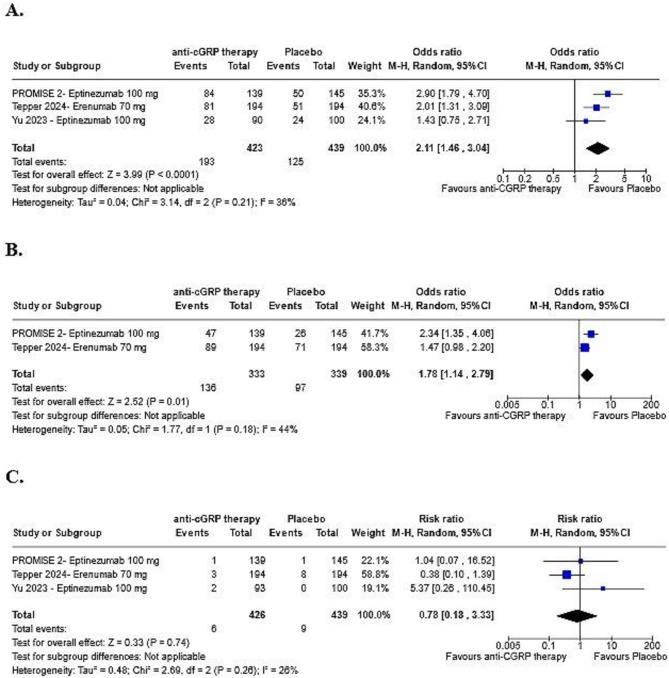
Three RCTs with 769 patients receiving standard-to-high dose anti-CGRP monoclonal antibodies (Eptinezumab and Erenumab) for ≥ 12 weeks were included. Anti-CGRP therapy significantly increased the likelihood of a ≥ 50% reduction in MMDs compared to placebo (OR: 2.43; 95% CI: 1.68-3.51; p < 0.00001). No substantial differences were found in TEAEs leading to discontinuation, nasopharyngitis, upper respiratory tract infections, or serious TEAEs between the anti-CGRP and placebo groups. The likelihood of MOH remission was approximately double in the anti-CGRP group (OR: 1.97; 95% CI: 1.40-2.78; p = 0.0001).
Standard-to-high dose anti-CGRP therapies (eptinezumab, erenumab) effectively reduce monthly migraine days and improve MOH remission rates with minimal adverse effects, showing good tolerability in CM patients with MOH.
使用靶向降钙素基因相关肽(CGRP)的单克隆抗体是慢性偏头痛(CM)的一种既定治疗方法。然而,其在药物过度使用性头痛(MOH)的CM患者中的疗效仍未得到充分探索,关于标准至高剂量(尤其是eptinezumab和erenumab)至少三个月的安全性和患者依从性的数据有限。
本研究旨在评估抗CGRP疗法(eptinezumab和erenumab)在CM和MOH患者中的疗效和安全性。具体而言,它评估了12周后每月偏头痛天数(MMD)的变化、导致停药的治疗中出现的不良事件(TEAE)风险、严重TEAE、常见不良反应以及6个月时MOH的缓解情况。
对PubMed、Cochrane和Scopus数据库进行系统检索,确定了评估标准或高剂量抗CGRP疗法在严格患有MOH的CM患者中的随机对照试验(RCT)。纳入的研究要求报告在≥12周后MMD减少≥50%、严重TEAE、导致停药的TEAE、常见不良反应以及6个月时MOH的缓解情况。使用I²统计量和随机效应模型评估异质性。
纳入了三项RCT,共769例患者接受标准至高剂量抗CGRP单克隆抗体(eptinezumab和erenumab)治疗≥12周。与安慰剂相比,抗CGRP疗法显著增加了MMD减少≥50%的可能性(OR:2.43;95%CI:1.68 - 3.51;p < 0.00001)。在抗CGRP组和安慰剂组之间,导致停药的TEAE、鼻咽炎、上呼吸道感染或严重TEAE方面未发现实质性差异。抗CGRP组MOH缓解的可能性约为两倍(OR:1.97;95%CI:1.40 - 2.78;p = 0.0001)。
标准至高剂量抗CGRP疗法(eptinezumab、erenumab)有效减少每月偏头痛天数并提高MOH缓解率,不良反应最小,在患有MOH的CM患者中显示出良好的耐受性。