Pathak Shresh, Tan Natalie, Vambutas Andrea
Northwell Health, 2000 Marcus Avenue, New Hyde Park, New York, NY, 11042, USA.
Feinstein Institutes for Medical Research, Manhasset, New York, NY, USA.
Mol Med. 2025 May 6;31(1):174. doi: 10.1186/s10020-025-01227-0.
Immune-mediated hearing loss (IMHL) patients (comprised of autoimmune inner ear disease (AIED) and sudden sensorineural hearing loss (SSNHL)) may be at higher risk for hearing loss following Coronavirus disease (COVID-19) infection and/or vaccination.
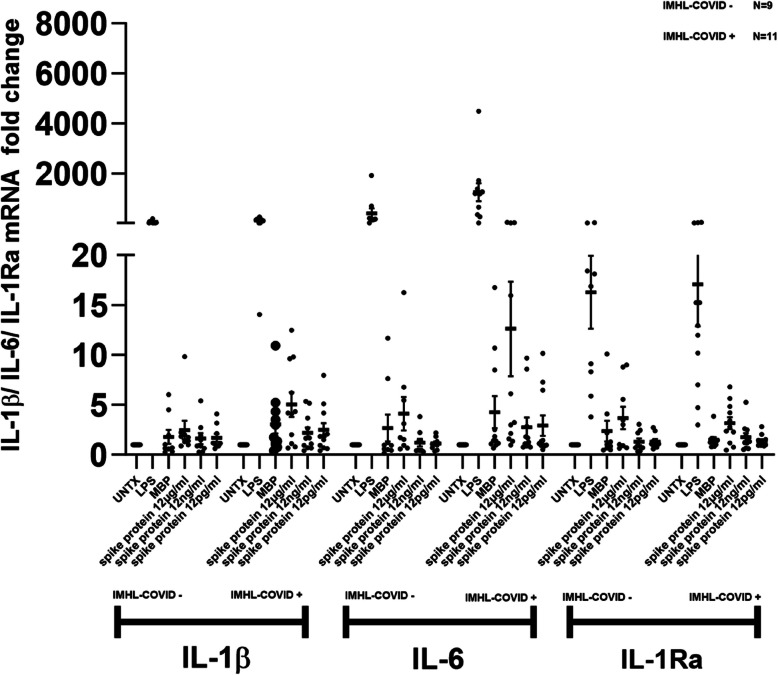
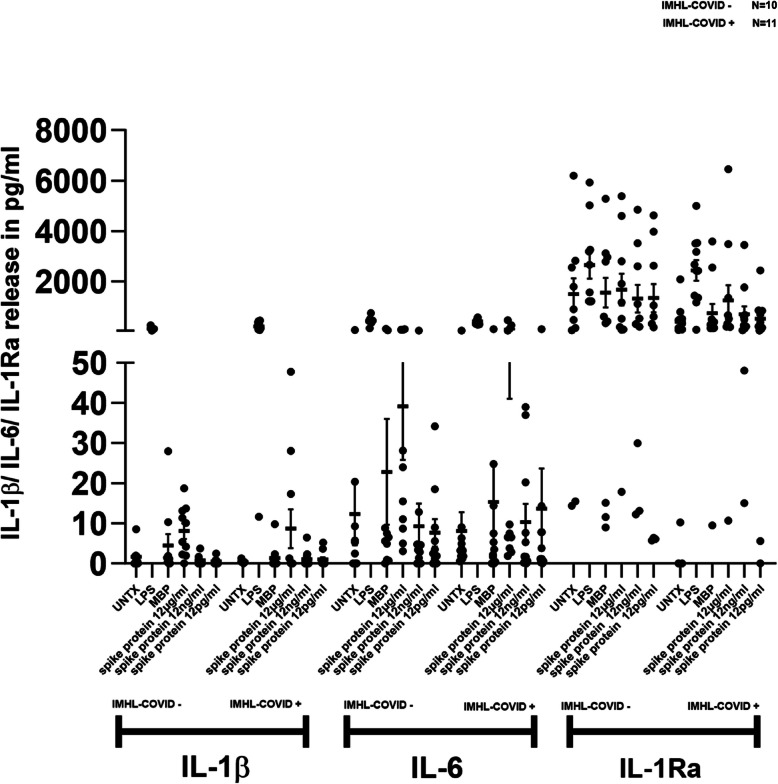
We compared inflammatory cytokine expression in response to SARS-CoV2 spike protein between two groups of patients with IMHL: IMHL patients that temporally demonstrated worsening SNHL following COVID vaccination or infection as compared to IMHL patients with worsening SNHL unrelated to COVID exposure: (IMHL-COVID ( +)) (n = 11) (IMHL-COVID (-)) (n = 10). In these two groups, we treated isolated PBMCs with increasing amounts of SARS-CoV-2 spike protein and compared responses to stimulation with positive and negative controls.
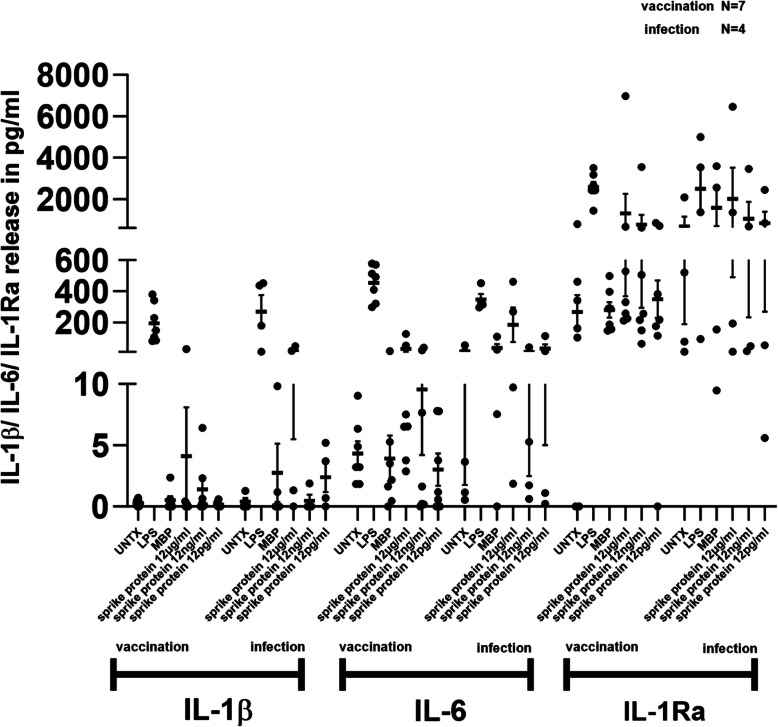
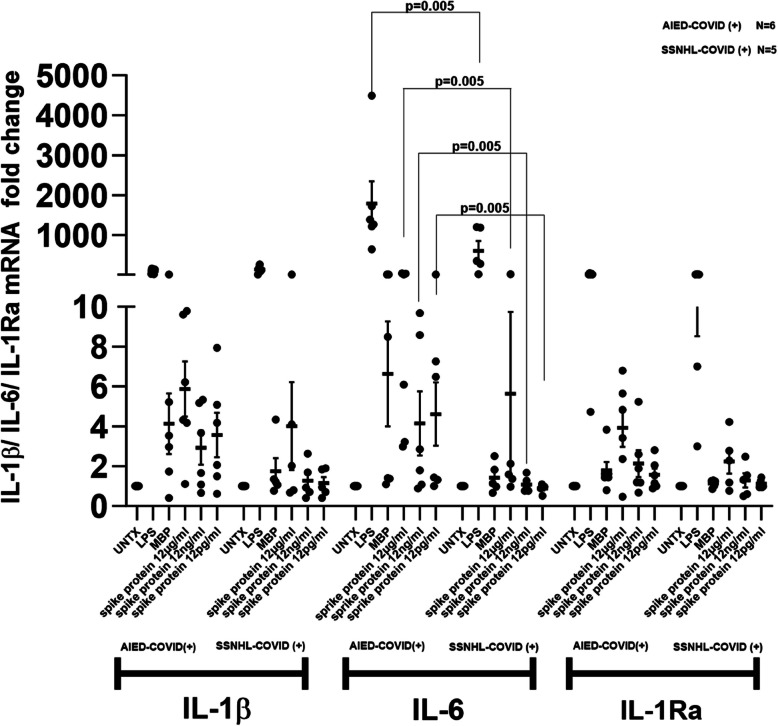
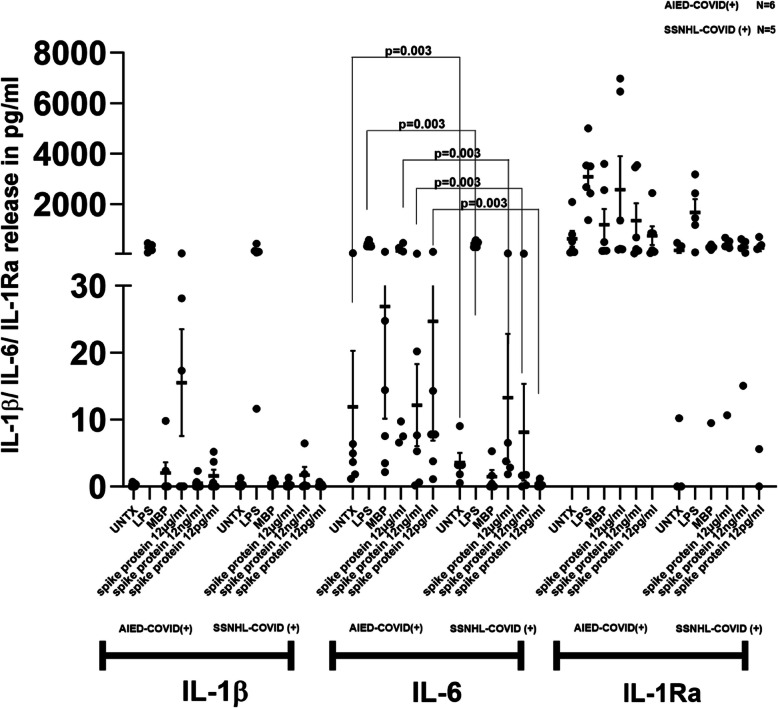
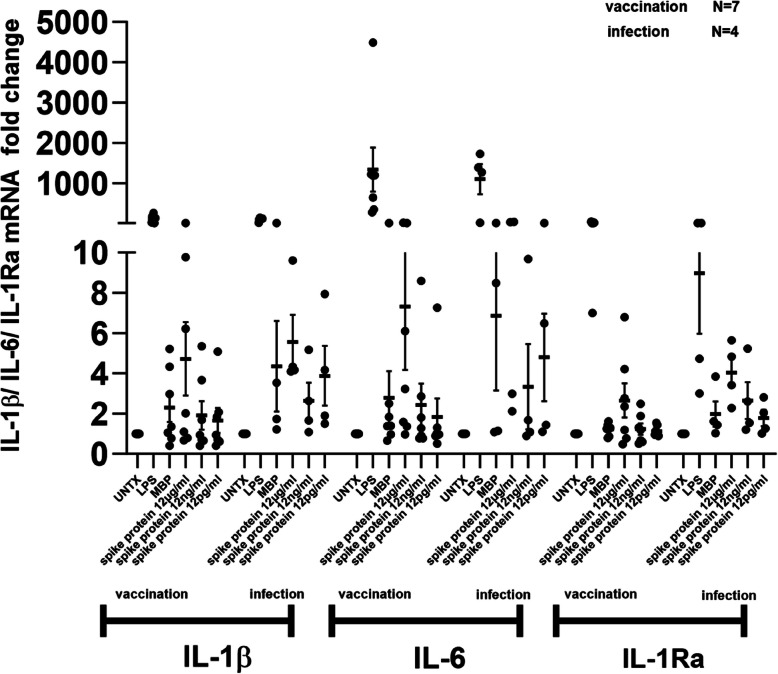
Peripheral Blood Mononuclear Cells (PBMC) from IMHL-COVID ( +) patients had increased expression and release of both IL-1β and IL-6 in response to spike protein as compared to IMHL-COVID (-) patients. However, when the IMHL-COVID ( +) group was broken down into AIED patients compared to SSNHL, it became apparent that the greatest responses were from the AIED patients (p < 0.005 for IL-6 mRNA expression and p < 0.003 for IL-6 release when compared between any two similar groups using Wilcoxon Rank-Sum Test). When we broke down the COVID ( +) group to infection versus vaccination, the immune responses in the infection group (N = 3 AIED, 1 SSNHL) were stronger.
COVID-19 exposure with reported changes in hearing sensitivity in IMHL patients resulted in pro-inflammatory responses in response to spike protein. The inflammatory responses were greatest in AIED patients, and greater following infection rather than vaccination. Therefore, based on these studies, we would recommend AIED patients take additional precautions to avoid COVID exposure. Furthermore, we do recommend COVID vaccination during periods of hearing stability, as the immune responses are even more robust in response to infection in this vulnerable group.
免疫介导性听力损失(IMHL)患者(包括自身免疫性内耳疾病(AIED)和突发性感音神经性听力损失(SSNHL))在感染和/或接种冠状病毒病(COVID-19)后可能有更高的听力损失风险。
我们比较了两组IMHL患者对严重急性呼吸综合征冠状病毒2(SARS-CoV2)刺突蛋白反应的炎性细胞因子表达:与听力损失恶化与COVID暴露无关的IMHL患者相比,在COVID疫苗接种或感染后暂时出现感音神经性听力损失恶化的IMHL患者:(IMHL-COVID(+))(n = 11)(IMHL-COVID(-))(n = 10)。在这两组中,我们用越来越多的SARS-CoV-2刺突蛋白处理分离的外周血单核细胞(PBMC),并将反应与阳性和阴性对照刺激进行比较。
与IMHL-COVID(-)患者相比,IMHL-COVID(+)患者的外周血单核细胞(PBMC)对刺突蛋白反应时白细胞介素-1β(IL-1β)和白细胞介素-6(IL-6)的表达和释放增加。然而,当将IMHL-COVID(+)组细分为AIED患者与SSNHL患者时,很明显最大反应来自AIED患者(使用Wilcoxon秩和检验在任何两个相似组之间比较时,IL-6 mRNA表达p < 0.005,IL-6释放p < 0.003)。当我们将COVID(+)组细分为感染组与疫苗接种组时,感染组(N = 3例AIED,1例SSNHL)的免疫反应更强。
据报道,IMHL患者在COVID-19暴露后听力敏感性发生变化,导致对刺突蛋白产生促炎反应。AIED患者的炎症反应最大,感染后的炎症反应大于疫苗接种后的炎症反应。因此,基于这些研究,我们建议AIED患者采取额外预防措施以避免COVID暴露。此外,我们确实建议在听力稳定期接种COVID疫苗,因为该弱势群体对感染的免疫反应更强。