Azad Arun A, Petrylak Daniel P, Iguchi Taro, Shore Neal D, Villers Arnauld, Gomez-Veiga Francisco, Alcaraz Antonio, Alekseev Boris, Szmulewitz Russell Z, Holzbeierlein Jeffrey, Rosbrook Brad, Ma Jie, Zohren Fabian, El-Chaar Nader N, Haas Gabriel P, Stenzl Arnulf, Armstrong Andrew J
Department of Medical Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia.
Department of Medical Oncology, Yale Cancer Center, New Haven, Connecticut.
JAMA Netw Open. 2025 May 1;8(5):e258751. doi: 10.1001/jamanetworkopen.2025.8751.
In men with metastatic hormone-sensitive prostate cancer (mHSPC), prostate-specific antigen (PSA) decline after treatment has been associated with improved survival. However, the data on PSA decline are limited in men with mHSPC after treatment with enzalutamide plus androgen deprivation therapy (ADT).
To evaluate the association of enzalutamide plus ADT in men with mHSPC by PSA level at study enrollment in individuals with prior ADT and by degree of PSA reduction with clinical end points.
DESIGN, SETTING, AND PARTICIPANTS: This post hoc secondary analysis was performed on data collected from the ARCHES multinational, double-blind, phase 3 randomized clinical trial. In the ARCHES trial, men with mHSPC were randomized between March 21, 2016, and January 12, 2018. Analyses were performed in October 2018 (median follow-up, 14.4 months; IQR, 11.2-17.7 months) and May 2021 (median follow-up, 44.6 months; IQR, 41.3-48.6 months).
Patients were randomized 1:1 to enzalutamide (160 mg/d) plus ADT or placebo plus ADT. ADT received for 3 to 6 months before study enrollment was permitted.
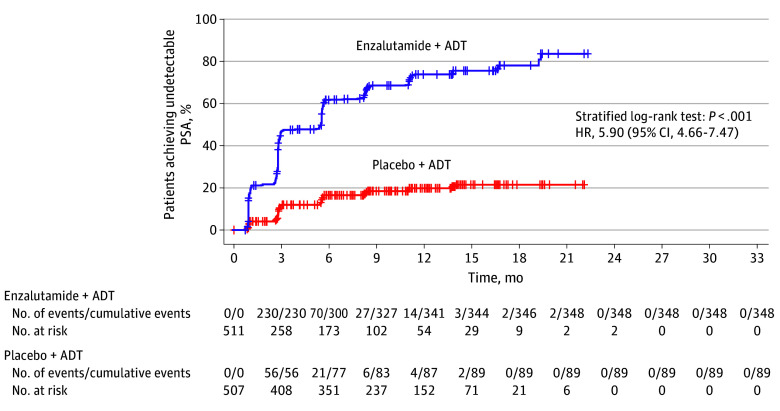
Radiographic progression-free survival (rPFS) and overall survival (OS) were correlated post hoc with PSA level at enrollment in patients with prior ADT and additionally with PSA decline at 6 months or undetectable PSA (<0.2 ng/mL) during study treatment.
A total of 1150 men (median age, 70 years; range, 46-92 years) were enrolled. Improvement in clinical outcomes such as rPFS was seen with enzalutamide plus ADT in men with PSA levels at enrollment of 0.2 to 4 ng/mL and above 4 ng/mL. Hazard ratios (HRs) for improved rPFS in men with PSA levels up to 0.2 ng/mL, above 0.2 to 4 ng/mL, and above 4 ng/mL were 0.59 (95% CI, 0.27-1.30), 0.32 (95% CI, 0.20-0.50), and 0.44 (95% CI, 0.32-0.62), respectively. Patients treated with enzalutamide plus ADT who achieved undetectable PSA had an 86.0% reduced risk of radiographic disease progression (HR, 0.14 [95% CI, 0.09-0.23]; P < .001) and a 76.0% reduced risk of death (HR, 0.24 [95% CI, 0.17-0.34]; P < .001).
In this secondary analysis of a randomized clinical trial, patients with mHSPC treated with enzalutamide plus ADT vs placebo plus ADT had improved clinical outcomes regardless of PSA level at enrollment. Undetectable PSA was associated with improved clinical outcomes with enzalutamide treatment. Future studies are required to further characterize the clinical utility of further treatment intensification among men with mHSPC for whom ADT plus enzalutamide fails to achieve undetectable PSA.
ClinicalTrials.gov Identifier: NCT02677896.
在转移性激素敏感性前列腺癌(mHSPC)男性患者中,治疗后前列腺特异性抗原(PSA)下降与生存率提高相关。然而,对于接受恩杂鲁胺加雄激素剥夺治疗(ADT)的mHSPC男性患者,关于PSA下降的数据有限。
通过既往接受ADT患者入组时的PSA水平以及PSA降低程度与临床终点的相关性,评估恩杂鲁胺加ADT对mHSPC男性患者的影响。
设计、背景和参与者:这项事后二次分析是基于ARCHES多中心、双盲、3期随机临床试验收集的数据进行的。在ARCHES试验中,mHSPC男性患者于2016年3月21日至2018年1月12日期间被随机分组。分析分别在2018年10月(中位随访时间14.4个月;四分位间距,11.2 - 17.7个月)和2021年5月(中位随访时间44.6个月;四分位间距,41.3 - 48.6个月)进行。
患者按1:1随机分组,分别接受恩杂鲁胺(160 mg/d)加ADT或安慰剂加ADT。允许在入组研究前接受3至6个月的ADT。
事后分析将影像学无进展生存期(rPFS)和总生存期(OS)与既往接受ADT患者入组时的PSA水平相关联,并额外与研究治疗期间6个月时的PSA下降情况或不可检测的PSA(<0.2 ng/mL)相关联。
共纳入1150名男性(中位年龄70岁;范围46 - 92岁)。对于入组时PSA水平为0.2至4 ng/mL及高于4 ng/mL的男性,恩杂鲁胺加ADT可改善rPFS等临床结局。入组时PSA水平高达0.2 ng/mL、高于0.2至4 ng/mL以及高于4 ng/mL的男性,rPFS改善的风险比(HR)分别为0.59(95%CI,0.27 - 1.30)、0.32(95%CI,0.20 - 0.50)和0.44(95%CI,0.32 - 0.62)。接受恩杂鲁胺加ADT治疗且PSA不可检测的患者,影像学疾病进展风险降低86.0%(HR,0.14 [95%CI,0.09 - 0.23];P <.001),死亡风险降低76.0%(HR,0.24 [95%CI,0.17 - 0.34];P <.001)。
在这项随机临床试验的二次分析中,与安慰剂加ADT相比,接受恩杂鲁胺加ADT治疗的mHSPC患者无论入组时的PSA水平如何,临床结局均得到改善。PSA不可检测与恩杂鲁胺治疗的临床结局改善相关。未来需要进一步研究,以进一步明确对于ADT加恩杂鲁胺治疗未能使PSA不可检测的mHSPC男性患者,进一步强化治疗的临床效用。
ClinicalTrials.gov标识符:NCT02677896。