Meyers Eline, De Rop Liselore, Gioveni Claudia, Engels Fien, Coen Anja, De Burghgraeve Tine, Digregorio Marina, Van Ngoc Pauline, De Clercq Nele, Buret Laëtitia, Coenen Samuel, Padalko Elizaveta, Duysburgh Els, Scholtes Beatrice, Verbakel Jan Y, Heytens Stefan, Cools Piet
Department of Diagnostic Sciences, Faculty of Medicine and Health Sciences, Ghent University, 9000 Ghent, Belgium.
LUHTAR-Leuven Unit for HTA Research, Department of Public Health and Primary Care, KU Leuven, 3000 Leuven, Belgium.
Vaccines (Basel). 2025 Apr 15;13(4):409. doi: 10.3390/vaccines13040409.
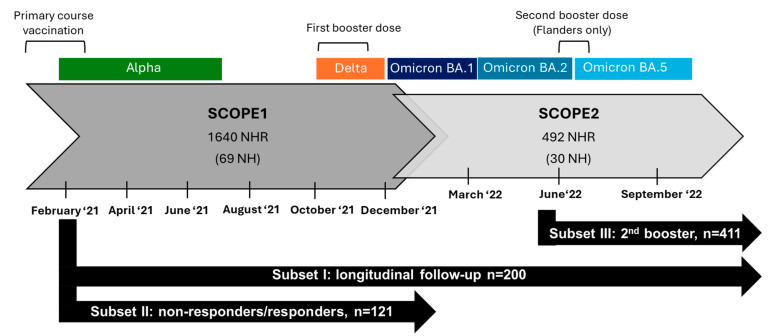
BACKGROUND/OBJECTIVES: This study mapped antibody dynamics across three COVID-19 vaccination rounds (primary course, first, and second booster with BNT162b2) in Belgian nursing home residents (NHRs).
Within a national SARS-CoV-2 serosurveillance study (February 2021-September 2022) across Belgian nursing homes, dried blood spots were collected, on which anti-spike SARS-CoV-2 IgG antibodies were quantified by ELISA in international units/mL (IU/mL). Sociodemographic data were collected at the study start and infection history and vaccination data at each sampling round.
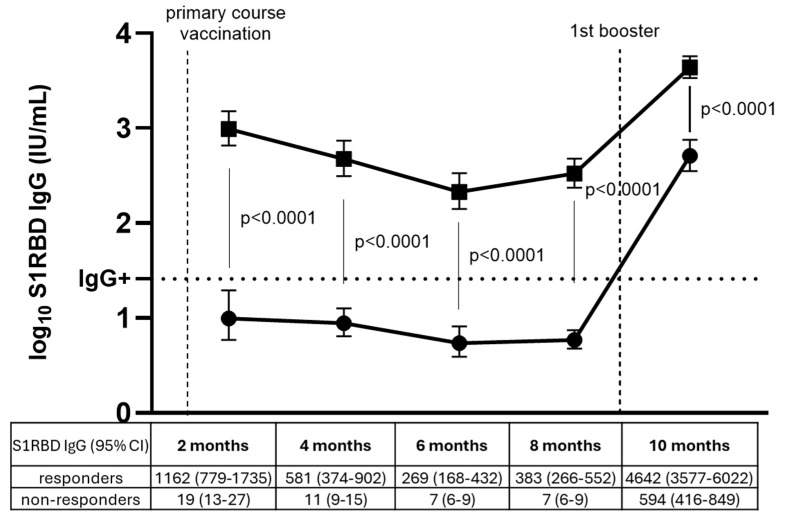
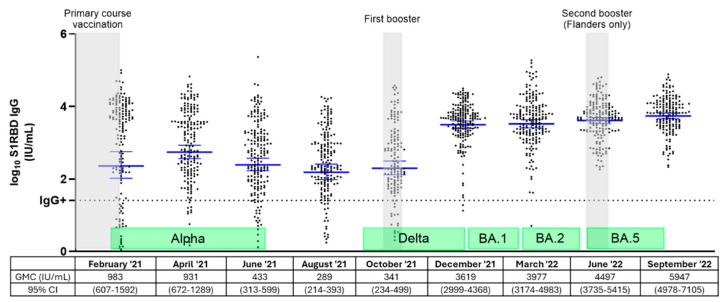
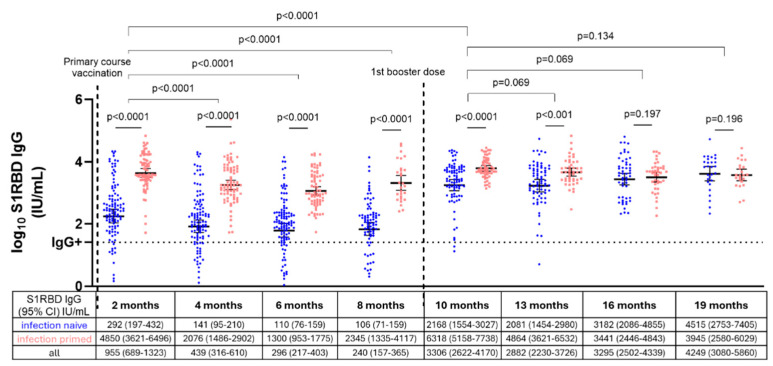
Infection-naïve NHRs had low antibody levels after primary course vaccination (geometric mean concentration (GMC) 292 IU/mL, 95% confidence interval (95% CI): 197-432), but increased tenfold after first booster (GMC 2168 IU/mL, 95% CI: 1554-3027). While antibodies among NHRs significantly declined within six months after primary vaccination ( < 0.0001), they remained stable for nine months post-booster ( > 0.05). Among primary vaccine non-responders, 92% (95% CI: 82-97%) developed antibodies after the first booster (GMC 594 IU/mL, 95% CI: 416-849), though tenfold lower than initial responders (GMC 4642 IU/mL, 95% CI: 3577-6022).
These findings demonstrate that NHRs require tailored vaccination, prioritizing repeated immunization to improve serological outcomes in poor responders such as infection-naive NHRs. Regular immune monitoring could aid in implementing evidence-based vaccine strategies, ensuring optimal protection for vulnerable populations against SARS-CoV-2 and other infectious threats.
背景/目的:本研究描绘了比利时养老院居民(NHRs)在三轮新冠病毒疫苗接种(基础免疫疗程、首次和第二次使用BNT162b2加强免疫)过程中的抗体动态变化。
在一项针对比利时养老院的全国性新冠病毒血清学监测研究(2021年2月至2022年9月)中,采集干血斑样本,通过酶联免疫吸附测定法(ELISA)以国际单位/毫升(IU/mL)为单位对新冠病毒刺突蛋白特异性IgG抗体进行定量分析。在研究开始时收集社会人口统计学数据,并在每次采样轮次收集感染史和疫苗接种数据。
未感染过新冠病毒的养老院居民在完成基础免疫疗程后抗体水平较低(几何平均浓度(GMC)为292 IU/mL,95%置信区间(95%CI):197 - 432),但在首次加强免疫后抗体水平增加了10倍(GMC为2168 IU/mL,95%CI:1554 - 3027)。虽然养老院居民在基础免疫接种后6个月内抗体水平显著下降(<0.0001),但在加强免疫后9个月内保持稳定(>0.05)。在基础疫苗接种无应答者中,92%(95%CI:82 - 97%)在首次加强免疫后产生了抗体(GMC为594 IU/mL,95%CI:416 - 849),尽管比初始应答者低10倍(GMC为4642 IU/mL,95%CI:3577 - 6022)。
这些研究结果表明,养老院居民需要进行个性化接种,优先考虑重复免疫,以改善像未感染过新冠病毒的养老院居民这类低应答者的血清学结果。定期免疫监测有助于实施基于证据的疫苗接种策略,确保为弱势群体提供针对新冠病毒和其他感染威胁的最佳保护。