Gajbhiye Raj, Solanke Rashmi, Tirpude Bhupesh, Deshpande Gayatri, Bhanarkar Hemant, Jadhao Ashutosh, Kursunge Vipin
General Surgery, Government Medical College Nagpur, Nagpur, IND.
Obstetrics and Gynecology, Government Medical College Nagpur, Nagpur, IND.
Cureus. 2025 Apr 7;17(4):e81832. doi: 10.7759/cureus.81832. eCollection 2025 Apr.
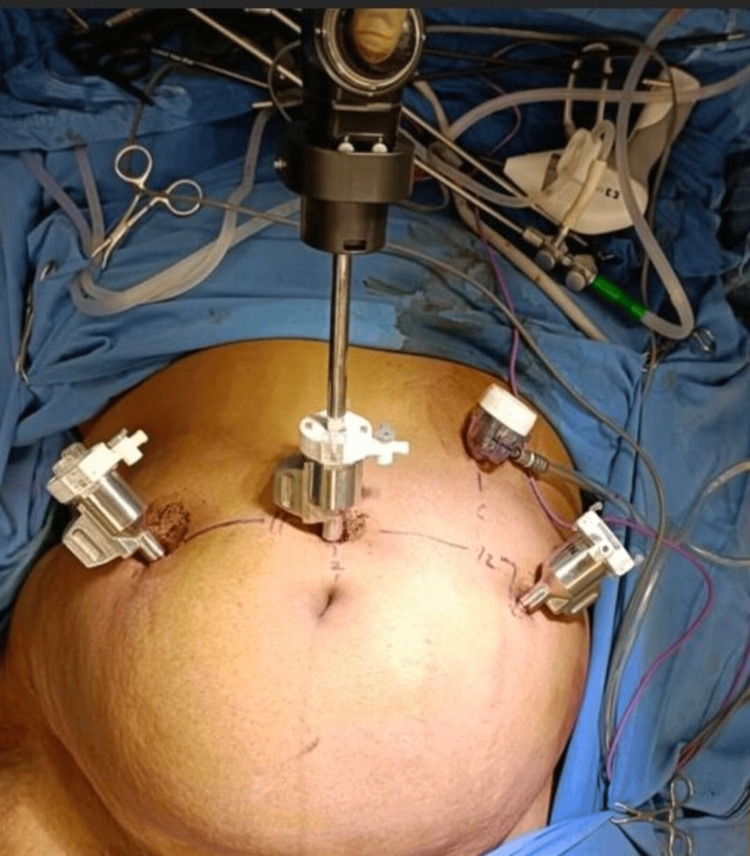
Background Minimally invasive hysterectomy approaches, including vaginal, laparoscopic, and robotic hysterectomy, offer advantages over laparotomic hysterectomy. However, vaginal hysterectomy is less feasible for patients with a large uterus, prior pelvic surgery, adnexal surgery requirements, or malignancy, making laparoscopy or robotic surgery preferable. The SSI Mantra robotic system (Sudhir Srivastava Innovations Pvt. Ltd., India) features an ergonomic open-faced console with a 32-inch 3D 4K monitor, a 23-inch 2D touch monitor for system control and DICOM applications, a head-tracking safety feature, and advanced ergonomic controls. This study evaluates the safety and efficacy of robotic hysterectomy using this indigenous system. Materials and methods From February to September 2024, 15 patients underwent robotic hysterectomy at Government Medical College, Nagpur. Patients were counseled about using the SSI Mantra robotic system and surgical risks, including possible conversion to laparotomy or robotic arm injury. The procedure followed a standard robotic port approach with accessory laparoscopic ports. Multiple surgeons performed the surgeries. The primary outcome was operative time, defined from incision start to closure. Additional data collected included patient intubation time, draping time, port placement, docking time, console time, surgical end time, patient out time, and estimated blood loss (fluid volume difference between irrigation and suction). Perioperative complications, readmissions, surgeon experience impact on operative time, conversion to laparotomy, hospital stay duration, hemoglobin drop, Visual Analogue Scale (VAS) pain scores, and intraoperative strategies (e.g., adhesiolysis, myomectomy) were analyzed. The weight of the excised uterus was also recorded. Results All 15 cases were successfully completed. The mean body mass index was 22.36 kg/m² (range: 19-25). The mean operative time (console use) was 169.41 minutes. Docking time improved from 25 minutes in the first case to five minutes by the 12th. The mean hospital stay was 4.5 days. The average uterine weight was 104.58 g (range: 25-250 g). Estimated blood loss averaged 129.16 mL (range: 30-400 mL). Vaginal cuff closure time was recorded in one case (20 minutes). The mean VAS pain score was 3.91. A hemoglobin drop occurred in four cases, but no postoperative blood transfusions were required. There were no conversions, major complications, or readmissions. Conclusions This study demonstrates that the indigenous robotic system provides enhanced ergonomics, seven degrees of freedom, ease of operation, and improved safety with a shorter learning curve for large uteri. Further studies are needed to assess postoperative and long-term outcomes.
背景 微创子宫切除术方法,包括经阴道、腹腔镜和机器人辅助子宫切除术,相较于开腹子宫切除术具有优势。然而,对于子宫较大、既往有盆腔手术史、有附件手术需求或患有恶性肿瘤的患者,经阴道子宫切除术可行性较低,使得腹腔镜或机器人手术更为可取。SSI Mantra机器人系统(印度Sudhir Srivastava创新私人有限公司)具有符合人体工程学的开放式控制台,配备32英寸3D 4K显示器、用于系统控制和DICOM应用的23英寸2D触摸显示器、头部跟踪安全功能以及先进的人体工程学控制装置。本研究评估使用该国产系统进行机器人辅助子宫切除术的安全性和有效性。
材料与方法 2024年2月至9月,15例患者在那格浦尔政府医学院接受了机器人辅助子宫切除术。向患者介绍了使用SSI Mantra机器人系统的情况以及手术风险,包括可能转为开腹手术或机器人手臂损伤。手术采用标准的机器人端口入路并辅以腹腔镜端口。由多名外科医生进行手术。主要结局指标为手术时间,定义为从切口开始至关闭的时间。收集的其他数据包括患者插管时间、铺巾时间、端口放置、对接时间、控制台操作时间、手术结束时间、患者离开手术室时间以及估计失血量(冲洗液与吸引液的液体量差值)。分析围手术期并发症、再次入院情况、外科医生经验对手术时间的影响、转为开腹手术情况、住院时间、血红蛋白下降情况、视觉模拟评分(VAS)疼痛评分以及术中策略(如粘连松解、肌瘤切除术)。还记录了切除子宫的重量。
结果 所有15例手术均成功完成。平均体重指数为22.36kg/m²(范围:19 - 25)。平均手术时间(控制台使用时间)为169.41分钟。对接时间从第一例的25分钟缩短至第12例的5分钟。平均住院时间为4.5天。平均子宫重量为104.58g(范围:25 - 250g)。估计平均失血量为129.16mL(范围:30 - 400mL)。有1例记录了阴道残端闭合时间(20分钟)。平均VAS疼痛评分为3.91。4例出现血红蛋白下降,但无需术后输血。无转为开腹手术、重大并发症或再次入院情况。
结论 本研究表明,该国产机器人系统具有增强的人体工程学设计、七个自由度、操作简便且安全性更高,对于大子宫而言学习曲线更短。需要进一步研究来评估术后及长期结局。