Ye Jian, Qin Shuyang S, Hughson Angela L, Hannon Gary, Salama Noah A, Vrooman Tara G, Lesch Maggie L, Lesser Sidney, Eckl Sarah L, Jewell Rachel, Benoodt Lauren, Mills Bradley N, Johnston Carl J, Lord Edith, Belt Brian A, Calvi Laura M, Linehan David, Luheshi Nadia, Eyles Jim, Gerber Scott A
Department of Surgery, University of Rochester Medical Center, Rochester, New York, USA.
Center for Tumor Immunology Research, University of Rochester Medical Center, Rochester, New York, USA.
J Immunother Cancer. 2025 May 7;13(5):e010820. doi: 10.1136/jitc-2024-010820.
Recent preclinical and clinical data suggest that leukemia inhibitory factor (LIF) is a potential target for various tumor types including pancreatic ductal adenocarcinoma as LIF is involved in multiple protumor processes including cancer stem cell maintenance, epithelial-mesenchymal transition (EMT), immunosuppression, and chemo/radioresistance. Anti-LIF antibody therapy has demonstrated safety and tolerability but limited efficacy in phase 1 clinical trial in advanced solid tumors. This prompted us to explore combination therapies, suggesting that LIF blockade, when combined with standard-of-care chemotherapy, radiotherapy, and/or immunotherapy, could present a promising therapeutic strategy.
We evaluated the impact of combining systemic inhibition of LIF/programmed death-ligand 1 (PD-L1) with localized stereotactic body radiotherapy (SBRT) on tumor progression across multiple murine orthotopic pancreatic tumor models and examined systemic antitumor immunity using a hepatic rechallenge model. The antitumor immune response was characterized throughflow cytometry and Luminex assays. To identify differentially expressed genes and signaling pathways following treatment, we performed bulk RNA sequencing on pancreatic tumors. Additionally, single-cell RNA sequencing was conducted to further examine changes in tumor-infiltrating immune cells and their signaling pathways.
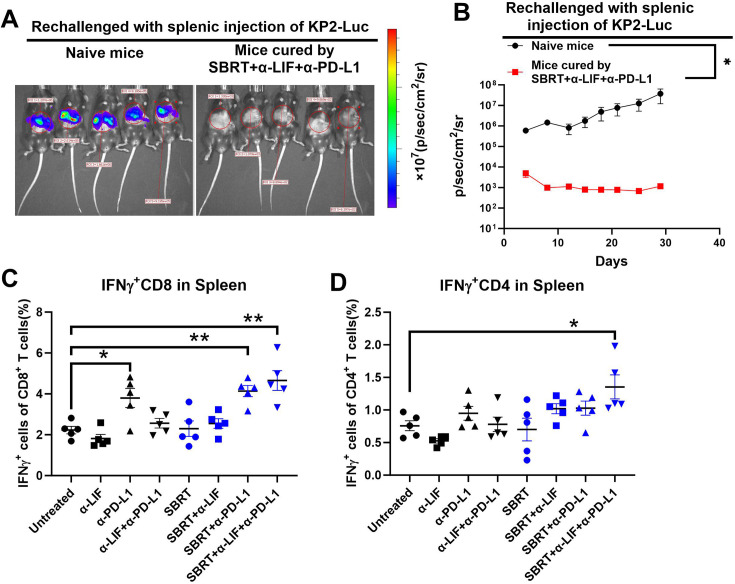
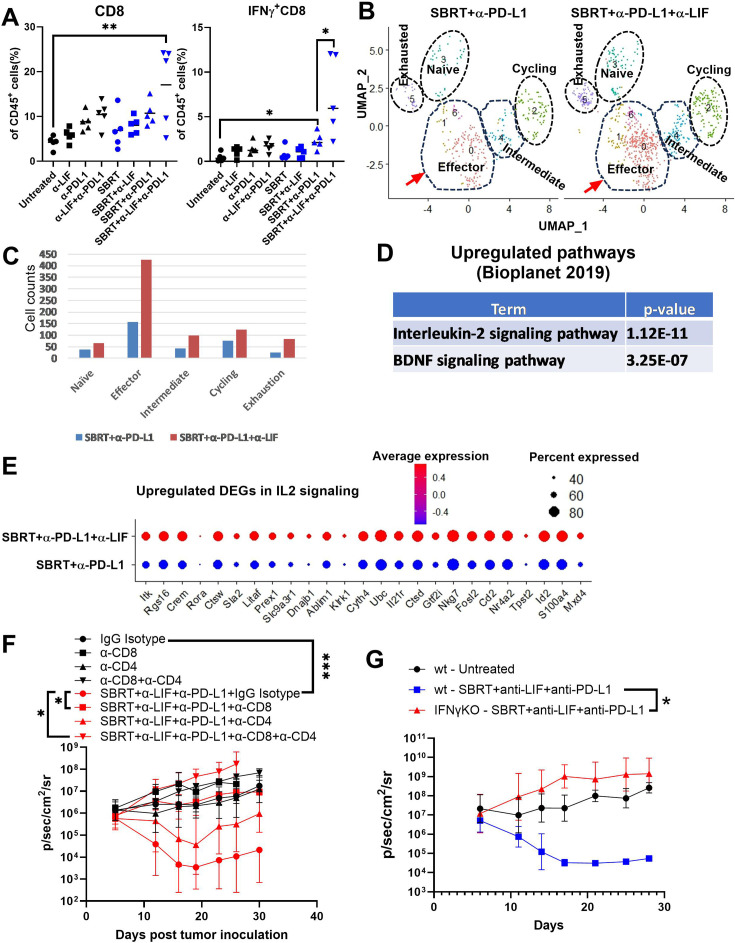
We showed that simultaneous inhibition of LIF and PD-L1 significantly amplified the antitumor efficacy of SBRT, resulting in extended survival. The triple therapy (SBRT+anti-LIF+anti-PD-L1) generated an immunostimulatory tumor microenvironment, characterized by a proinflammatory shift in the cytokine/chemokine profile, increased infiltration of effector CD8 T cells, and upregulated activation or maturation signals in tumor-infiltrating CD8 T cells and macrophages. The beneficial effects of triple therapy were mostly abrogated by depletion of CD8 T cells. In addition, triple therapy downregulated pathways related to tumor stemness, proliferation, and metabolism, and reduced EMT. Importantly, the combination of local SBRT treatment with systemic LIF and PD-L1 blockade resulted in long-term systemic antitumor memory.
最近的临床前和临床数据表明,白血病抑制因子(LIF)是包括胰腺导管腺癌在内的多种肿瘤类型的潜在靶点,因为LIF参与多个促肿瘤过程,包括癌症干细胞维持、上皮-间质转化(EMT)、免疫抑制以及化疗/放疗抗性。抗LIF抗体疗法在晚期实体瘤的1期临床试验中已证明具有安全性和耐受性,但疗效有限。这促使我们探索联合疗法,表明LIF阻断与标准护理化疗、放疗和/或免疫疗法联合使用时,可能是一种有前景的治疗策略。
我们评估了在多个小鼠原位胰腺肿瘤模型中,将LIF/程序性死亡配体1(PD-L1)的全身抑制与局部立体定向体部放疗(SBRT)相结合对肿瘤进展的影响,并使用肝脏再激发模型检查全身抗肿瘤免疫。通过流式细胞术和Luminex分析来表征抗肿瘤免疫反应。为了确定治疗后差异表达的基因和信号通路,我们对胰腺肿瘤进行了批量RNA测序。此外,进行了单细胞RNA测序,以进一步检查肿瘤浸润免疫细胞的变化及其信号通路。
我们表明,同时抑制LIF和PD-L1可显著增强SBRT的抗肿瘤疗效,从而延长生存期。三联疗法(SBRT+抗LIF+抗PD-L1)产生了免疫刺激的肿瘤微环境,其特征是细胞因子/趋化因子谱向促炎转变、效应CD8 T细胞浸润增加,以及肿瘤浸润CD8 T细胞和巨噬细胞中的激活或成熟信号上调。三联疗法的有益效果在很大程度上被CD8 T细胞耗竭所消除。此外,三联疗法下调了与肿瘤干性、增殖和代谢相关的通路,并减少了EMT。重要的是,局部SBRT治疗与全身LIF和PD-L1阻断相结合可产生长期的全身抗肿瘤记忆。