van Tetering Anne A C, de Vries Ella L, Ntuyo Peter, van den Heuvel E R, Fransen Annemarie F, van der Hout-van der Jagt M Beatrijs, Namagembe Imelda, Byamugisha Josaphat, Oei S Guid
Department of Electrical Engineering, Eindhoven University of Technology, Eindhoven, The Netherlands.
Department of Obstetrics and Gynaecology, Amphia Ziekenhuis, Breda, The Netherlands.
JMIR Med Educ. 2025 May 9;11:e54911. doi: 10.2196/54911.
Emergency obstetric simulation-based training has increasingly been used to improve emergency obstetric care provision in sub-Saharan Africa. For determining the optimal methodology for effective training sessions in resource-constrained settings, it is crucial to conduct high-quality research.
We aim to investigate the impact of a train-the-trainer model for providing technology-enhanced, mono-professional, simulation-based training in obstetrics in a resource-constrained setting on maternal and perinatal outcomes.
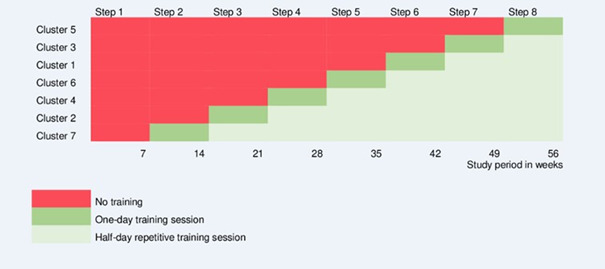
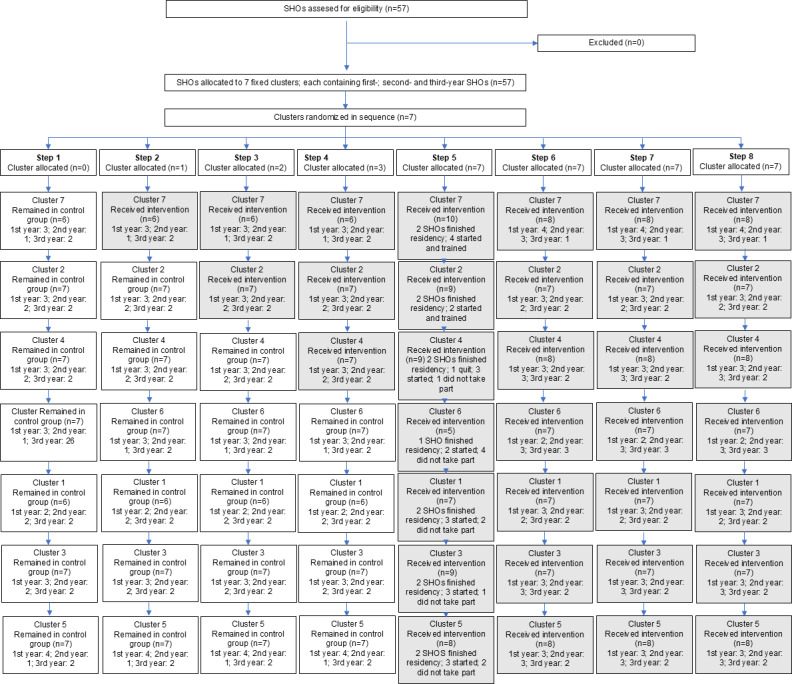
A stepped-wedge cluster randomized trial was conducted from October 2014 until March 2016 at the medium- to high-risk ward at Mulago National Referral Hospital, Uganda, with an annual delivery rate of over 23,000. The intervention consisted of a train-the-trainer model in which training was cascaded down from master trainers to local facilitators (obstetric senior staff members) to learners (senior house officers). The training of senior house officers was provided to 7 fixed clusters by a computer-generated random sequential roll-out. The training comprised a 1-day (8 h), mono-professional, simulation-based training in obstetrics, and half-day repetition training sessions targeted at every 7 weeks. Both medical technical skills and teamwork skills were taught. The primary outcome comprised a combined maternal and perinatal mortality rate. Secondary outcomes comprised the maternal mortality rate, the perinatal mortality rate, the percentage of births by vacuum extraction and cesarean section, and the Weighted Adverse Outcome Score.
Overall, there were 17,496 births. The combined mortality rate was 9.05% (95% CI 8.37%-9.77%) in the intervention group, and 8.73% (95% CI 8.21%-9.28%) in the control group (odds ratio [OR] 0.98, 95% CI 0.86-1.12; P=.81). No statistically significant change was found in the maternal mortality rate (OR 0.80, 95% CI 0.27-2.32; P=.68) or the perinatal mortality rate (OR 0.99, 95% CI 0.87-1.13; P=.87). This study did not identify any difference in the percentage of vacuum extractions, the percentage of cesarean sections, or Weighted Adverse Outcome Scores.
This train-the-trainer model for providing technology-enhanced, mono-professional, simulation-based training in obstetrics was not able to change maternal and perinatal mortality outcomes. This study, in combination with literature, suggests that future research should consider multiprofessional team training in obstetrics involving all staff within their units.
基于模拟的产科急救培训在撒哈拉以南非洲越来越多地被用于改善产科急救服务。对于在资源有限的环境中确定有效培训课程的最佳方法,开展高质量研究至关重要。
我们旨在调查在资源有限的环境中,采用培训培训师模式提供技术增强型、单一专业、基于模拟的产科培训对孕产妇和围产儿结局的影响。
2014年10月至2016年3月在乌干达穆拉戈国家转诊医院的中高风险病房进行了一项阶梯楔形整群随机试验,该病房年分娩率超过23000例。干预措施包括培训培训师模式,即培训从主培训师逐步传递给当地协调员(产科高级 staff 成员)再到学习者(高级住院医师)。通过计算机生成的随机顺序推出,为7个固定整群的高级住院医师提供培训。培训包括为期1天(8小时)的单一专业、基于模拟的产科培训,以及每7周进行一次的半天重复培训课程。同时教授医疗技术技能和团队合作技能。主要结局包括孕产妇和围产儿合并死亡率。次要结局包括孕产妇死亡率、围产儿死亡率、真空吸引分娩和剖宫产的百分比,以及加权不良结局评分。
总体而言,共有17496例分娩。干预组的合并死亡率为9.05%(95%CI 8.37%-9.77%),对照组为8.73%(95%CI 8.21%-9.28%)(优势比[OR]0.98,95%CI 0.86-1.12;P = 0.81)。孕产妇死亡率(OR 0.80,95%CI 0.27-2.32;P = 0.68)或围产儿死亡率(OR 0.99,95%CI 0.87-1.13;P = 0.87)未发现有统计学意义的变化。本研究未发现真空吸引分娩百分比、剖宫产百分比或加权不良结局评分有任何差异。
这种提供技术增强型、单一专业、基于模拟的产科培训的培训培训师模式未能改变孕产妇和围产儿死亡率结局。本研究结合文献表明,未来的研究应考虑对产科涉及单位内所有 staff 的多专业团队进行培训。