Institute for Global Health Sciences, University of California San Francisco, San Francisco, CA, USA; Department of Obstetrics, Gynecology, and Reproductive Sciences, University of California San Francisco, San Francisco, CA, USA.
Center for Clinical Research, Kenya Medical Research Institute, Nairobi, Kenya.
Lancet Glob Health. 2020 Aug;8(8):e1061-e1070. doi: 10.1016/S2214-109X(20)30232-1.
Although gains in newborn survival have been achieved in many low-income and middle-income countries, reductions in stillbirth and neonatal mortality have been slow. Prematurity complications are a major driver of stillbirth and neonatal mortality. We aimed to assess the effect of a quality improvement package for intrapartum and immediate newborn care on stillbirth and preterm neonatal survival in Kenya and Uganda, where evidence-based practices are often underutilised.
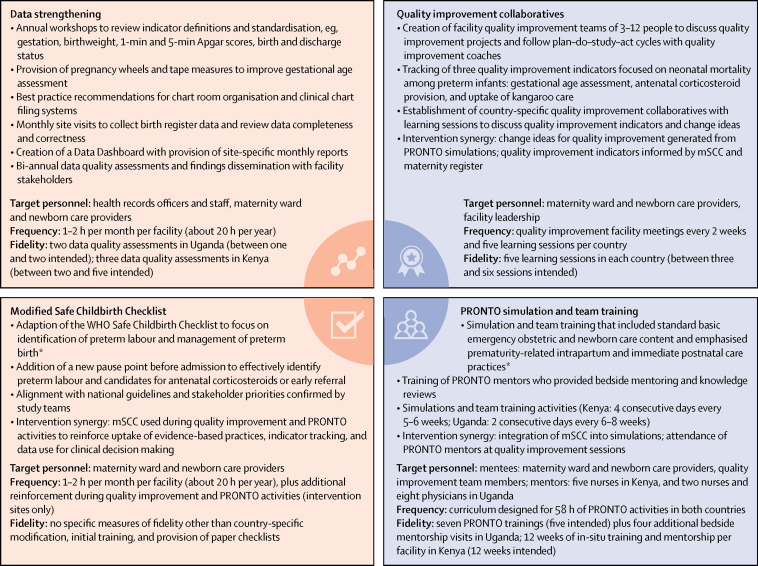
This unblinded cluster-randomised controlled trial was done in western Kenya and eastern Uganda at facilities that provide 24-h maternity care with at least 200 births per year. The study assessed outcomes of low-birthweight and preterm babies. Eligible facilities were pair-matched and randomly assigned (1:1) into either the intervention group or the control group. All facilities received maternity register data strengthening and a modified WHO Safe Childbirth Checklist; facilities in the intervention group additionally received provider mentoring using PRONTO simulation and team training as well as quality improvement collaboratives. Liveborn or fresh stillborn babies who weighed between 1000 g and 2500 g, or less than 3000 g with a recorded gestational age of less than 37 weeks, were included in the analysis. We abstracted data from maternity registers for maternal and birth outcomes. Follow-up was done by phone or in person to identify the status of the infant at 28 days. The primary outcome was fresh stillbirth and 28-day neonatal mortality. This trial is registered with ClinicalTrials.gov, NCT03112018.
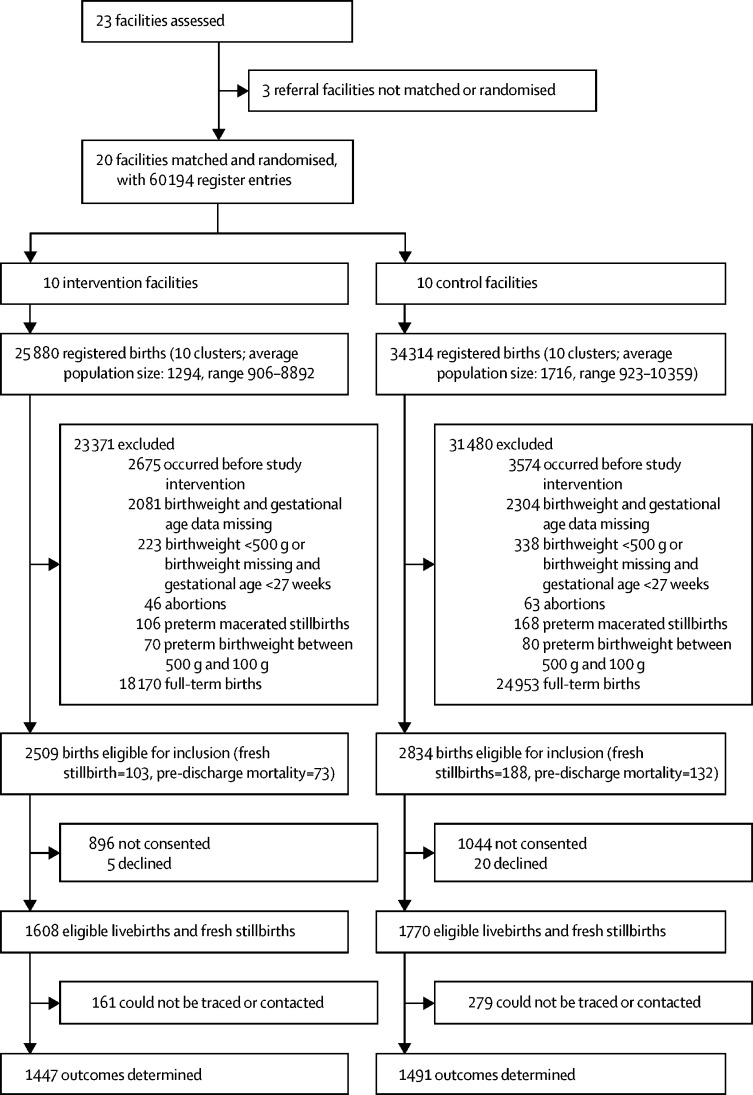
Between Oct 1, 2016, and April 30, 2019, 20 facilities were randomly assigned to either the intervention group (n=10) or the control group (n=10). Among 5343 eligible babies in these facilities, we assessed outcomes of 2938 newborn and fresh stillborn babies (1447 in the intervention and 1491 in the control group). 347 (23%) of 1491 infants in the control group were stillborn or died in the neonatal period compared with 221 (15%) of 1447 infants in the intervention group at 28 days (odds ratio 0·66, 95% CI 0·54-0·81). No harm or adverse effects were found.
Fresh stillbirth and neonatal mortality among low-birthweight and preterm babies can be decreased using a package of interventions that reinforces evidence-based practices and invests in health system strengthening.
Bill & Melinda Gates Foundation.
尽管许多低收入和中等收入国家已经在新生儿存活率方面取得了进展,但死产率和新生儿死亡率的下降速度却较为缓慢。早产并发症是导致死产和新生儿死亡的主要原因。本研究旨在评估在肯尼亚和乌干达实施产时和新生儿即刻护理质量改进措施对降低死产率和早产儿存活率的影响,这两个国家的基本实践往往未得到充分利用。
这是一项在肯尼亚西部和乌干达东部的 24 小时母婴保健设施中进行的、非盲、集群随机对照试验。这些设施每年至少有 200 例分娩。该研究评估了低出生体重和早产儿的结局。符合条件的设施进行配对,并按照 1:1 的比例随机分配(干预组或对照组)。所有设施均接受了孕产妇登记数据强化和经过改良的世界卫生组织安全分娩清单;干预组的设施还接受了 PRONTO 模拟和团队培训以及质量改进合作的提供者指导。纳入分析的是出生体重为 1000 克至 2500 克之间或出生体重小于 3000 克但记录的胎龄小于 37 周的有活力的或新鲜的死产儿。我们从产妇登记处获取了产妇和分娩结局的数据。通过电话或亲自随访,在 28 天时确定婴儿的状态。主要结局为新鲜死产和 28 天新生儿死亡率。该试验在 ClinicalTrials.gov 注册,编号为 NCT03112018。
2016 年 10 月 1 日至 2019 年 4 月 30 日,20 家设施被随机分配到干预组(n=10)或对照组(n=10)。在这些设施中,5343 名符合条件的婴儿中,我们评估了 2938 名新生儿和新鲜死产儿的结局(干预组 1447 名,对照组 1491 名)。对照组中 347(23%)名 1491 名婴儿在新生儿期死亡或死亡,而干预组中 1447 名婴儿中有 221(15%)名在 28 天时死亡(比值比 0.66,95%CI 0.54-0.81)。未发现任何伤害或不良影响。
通过强化基于证据的实践和投资于卫生系统强化的干预措施包,可以降低低出生体重和早产儿的新鲜死产率和新生儿死亡率。
比尔及梅琳达·盖茨基金会。