Zhang Jiani, Yan Jincao, Shi Yunke, Li Xingxing, Xin Youqing, Zhang Ning
School of Public Health, Capital Medical University, Beijing, 100069, P.R. China.
Chuiyangliu Hospital affiliated to Tsinghua University, Beijing, 100022, P.R. China.
BMC Public Health. 2025 May 9;25(1):1722. doi: 10.1186/s12889-025-22979-8.
Amid efforts to develop primary healthcare, China has been working to establish an integrated care system through the county medical community model, incorporating capitation payment to improve chronic disease management. This study investigates the impact of capitation payment reform on diabetes-related healthcare service behaviors across different levels of healthcare facilities within the county medical community.
We conducted interrupted time series analysis to evaluate the changes in healthcare service behavior before and after the implementation of the capitation model. Using F County, as the sample area, we collected outpatient reimbursement records of type 2 diabetes mellitus (T2DM) patients from six townships that initiated reform in April 2015. The dataset, covering January 2014 to December 2019, includes 49,326 records from primary healthcare facilities and 1,628 from county hospitals, with information on medical costs, service items, and other details.
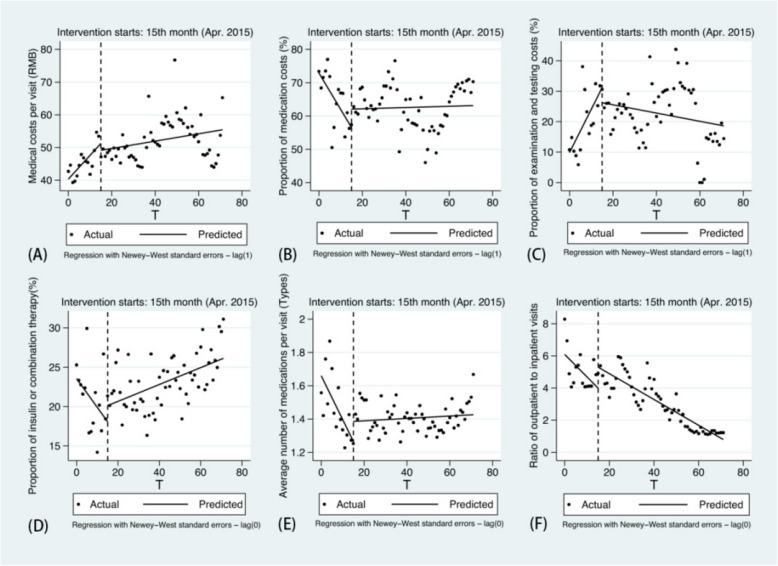
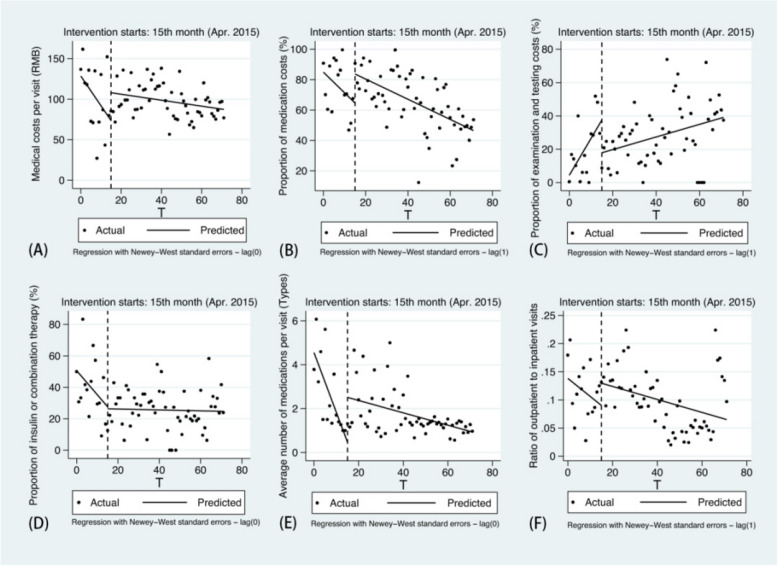
Following the implementation of capitation, both the average medical costs per visit and proportion of examination and testing costs showed a deceleration in growth in primary healthcare facilities (-0.615, p < 0.05; -1.554, p < 0.01). The proportion of medication costs, the proportion of insulin or combination therapy and the average number of medications exhibited a significant downward trend prior to the reform, while all reversed to upward trends after reform. In county hospitals, the proportion of medication costs increased by 19.115% immediately post-reform, and both the level and slope of average number of medications significantly rose (2.041, p < 0.01; 0.244, p < 0.01). Although the proportion of examination and testing costs increased before the reform, both the instantaneous level and the trend declined afterward (-19.684, p < 0.05; -1.833, p < 0.05).
In the sample area, the average medical costs for T2DM outpatients were effectively controlled after the capitation reform. Township health centers showed improved standardization in prescribing practices, while county hospitals focused more on comprehensive examinations and testing services. Medication prescription intensity increased across all facilities, contributing to enhanced chronic disease management.
在发展基层医疗保健的努力中,中国一直致力于通过县域医共体模式建立整合式医疗体系,并引入按人头付费以改善慢性病管理。本研究调查了按人头付费改革对县域医共体内不同层级医疗机构中与糖尿病相关的医疗服务行为的影响。
我们进行了中断时间序列分析,以评估按人头付费模式实施前后医疗服务行为的变化。以F县为样本地区,我们收集了2015年4月启动改革的6个乡镇中2型糖尿病(T2DM)患者的门诊报销记录。该数据集涵盖2014年1月至2019年12月,包括基层医疗机构的49326条记录和县级医院的1628条记录,包含医疗费用、服务项目及其他详细信息。
实施按人头付费后,基层医疗机构每次就诊的平均医疗费用以及检查和检验费用的占比均呈现增长减速(-0.615,p<0.05;-1.554,p<0.01)。改革前药品费用占比、胰岛素或联合治疗占比以及平均用药数量呈显著下降趋势,而改革后均转为上升趋势。在县级医院,改革后药品费用占比立即增加了19.115%,平均用药数量的水平和斜率均显著上升(2.041,p<0.01;0.244,p<0.01)。虽然改革前检查和检验费用占比增加,但之后瞬时水平和趋势均下降(-19.684,p<0.05;-1.833,p<0.05)。
在样本地区,按人头付费改革后T2DM门诊患者的平均医疗费用得到有效控制。乡镇卫生院的处方行为规范性有所改善,而县级医院则更侧重于综合检查和检验服务。所有医疗机构的用药处方强度均有所增加,有助于加强慢性病管理。