Wang Xiuri, Liang Lingyan, Liang Yunxiao, Hu Liuyang
Department of Gastroenterology, The People's Hospital of Guangxi Zhuang Autonomous Region, Guangxi Academy of Medical Sciences, Nanning, 530016, China.
Department of Radiology, The People's Hospital of Guangxi Zhuang Autonomous Region, Guangxi Academy of Medical Sciences, Nanning, 530016, China.
BMC Infect Dis. 2025 May 13;25(1):694. doi: 10.1186/s12879-025-11056-5.
Nocardial brain abscesses are extremely rare and predominantly affect immunocompromised patients, exhibiting a high overall mortality rate. Tuberculosis infections, although they can occur in immunocompetent individuals, are more prevalent in those with compromised immune systems. Tuberculous meningitis (TBM), the most severe manifestation of tuberculosis, is associated with a high fatality rate. Co-infection with both pathogens is unusual. To our knowledge, this is the first reported case of multiple brain abscesses caused by Nocardia abscessus (N. abscessus) in a young immunocompetent patient, complicated by tuberculous meningitis.
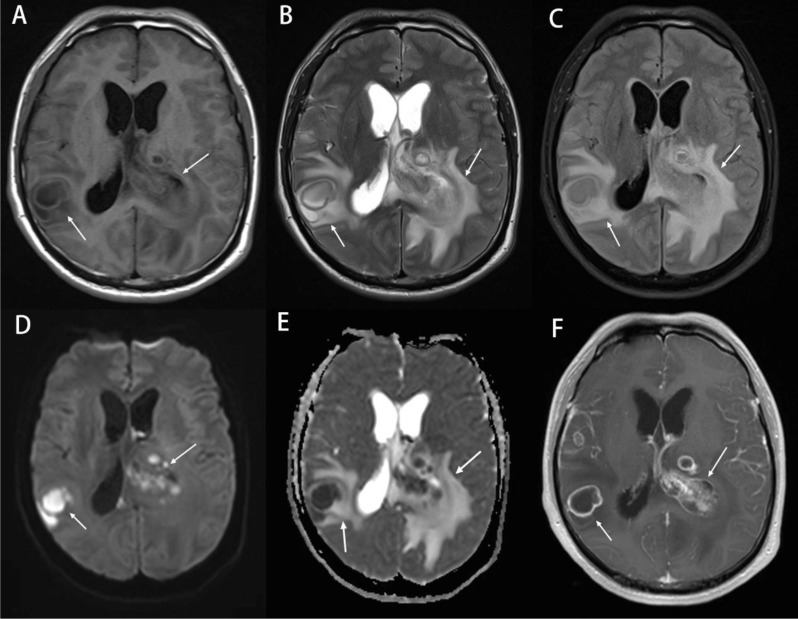
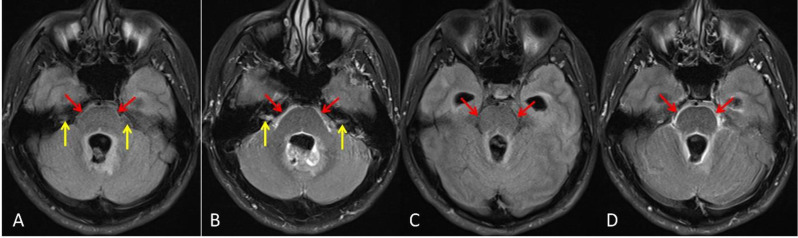
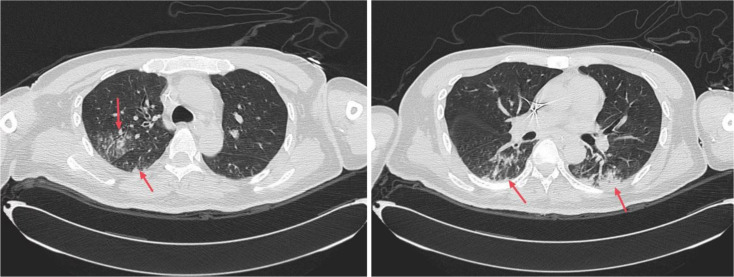
A 34-year-old male patient initially presented with a week-long history of headaches, predominantly localized in the bilateral frontal region. Additionally, the patient experienced fever, and due to the recurrence of these symptoms, he was admitted to the hospital. Chest computed tomography (CT) scans revealed bilateral pneumonia, and brain magnetic resonance imaging (MRI) strongly suggested the presence of multiple brain abscesses accompanied by meningitis. On the fourth day of hospitalization, the patient's condition deteriorated, becoming lethargic with severe headaches. His body temperature spiked to 39.5 °C, and signs of elevated intracranial pressure emerged. Subsequently, he underwent neuro-navigation-assisted resection of deep lesions, ventriculostomy for external drainage, and drainage of abscesses. The next day, cerebrospinal fluid (CSF) Xpert MTB/RIF testing yielded positive results for multiple probes and the Mycobacterium tuberculosis (MTB) complex. Pus cultures and sequencing further confirmed an N. abscessus infection. Consequently, the patient was diagnosed with multiple brain abscesses caused by N. abscessus, complicated by tuberculous meningitis. We administered TMP-SMX, imipenem-cilastatin, and intravenous linezolid for the management of nocardial brain abscesses infections, while continuing decompressive ventricular drainage. For empiric treatment of tuberculous meningitis, the patient was started on isoniazid 600 mg/day via intravenous injection, rifampicin 600 mg/day orally, pyrazinamide 1500 mg/day (divided into three oral doses), ethambutol 750 mg/day orally, and dexamethasone at an initial dose of 0.4 mg/kg/day, with a planned gradual reduction starting one week later. Despite 10 days of treatment, the patient showed no significant clinical improvement in the infection, and hydrocephalus worsened. On the 16th day of admission, emergency external ventricular drain placement was performed, and intrathecal amikacin was administered to combat the nocardial brain abscesses. Unfortunately, by the 39th day of admission, the patient's infection continued to progress, eventually succumbing to septic shock and resulting in death.
Nocardial brain abscesses are associated with a high mortality rate, especially among immunocompromised patients and those with multiple abscesses. Prompt diagnosis, aggressive surgical intervention, and sensitive antibiotic treatment offer the best prospects for curing nocardiosis. Tuberculous meningitis, the most lethal manifestation of Mycobacterium tuberculosis infection, often leads to severe outcomes primarily due to delayed diagnosis and treatment. The GeneXpert/RIF assay, an emerging diagnostic tool, provides a more sensitive and rapid means of detecting TBM. For patients with a high clinical suspicion of TBM, empirical anti-tuberculosis treatment should be initiated immediately. Timely and accurate management, coupled with continuous monitoring of the patient's condition, is crucial for achieving a favorable prognosis.
Not applicable.
诺卡菌性脑脓肿极为罕见,主要影响免疫功能低下的患者,总体死亡率较高。结核病感染虽然可发生于免疫功能正常者,但在免疫系统受损者中更为常见。结核性脑膜炎(TBM)是结核病最严重的表现形式,病死率很高。两种病原体合并感染并不常见。据我们所知,这是首例在年轻免疫功能正常患者中由脓肿诺卡菌(N. abscessus)引起的多发性脑脓肿合并结核性脑膜炎的报道病例。
一名34岁男性患者最初出现为期一周的头痛病史,主要位于双侧额部。此外,患者有发热症状,因这些症状反复出现而入院。胸部计算机断层扫描(CT)显示双侧肺炎,脑部磁共振成像(MRI)强烈提示存在多发性脑脓肿并伴有脑膜炎。住院第4天,患者病情恶化,变得嗜睡且头痛剧烈。体温飙升至39.5℃,出现颅内压升高迹象。随后,他接受了神经导航辅助下深部病变切除术、脑室造瘘术进行外引流以及脓肿引流。次日,脑脊液(CSF)Xpert MTB/RIF检测多个探针及结核分枝杆菌(MTB)复合体呈阳性结果。脓液培养和测序进一步证实为脓肿诺卡菌感染。因此,患者被诊断为脓肿诺卡菌引起的多发性脑脓肿,合并结核性脑膜炎。我们给予复方磺胺甲恶唑、亚胺培南 - 西司他丁和静脉注射利奈唑胺治疗诺卡菌性脑脓肿感染,同时继续进行减压性脑室引流。为经验性治疗结核性脑膜炎,患者开始静脉注射异烟肼600mg/天、口服利福平600mg/天、口服吡嗪酰胺1500mg/天(分三次口服)、口服乙胺丁醇750mg/天,地塞米松初始剂量为0.4mg/kg/天,计划一周后逐渐减量。尽管治疗了10天,患者感染情况未出现明显临床改善,脑积水加重。入院第16天,进行了紧急体外脑室引流,并鞘内注射阿米卡星以对抗诺卡菌性脑脓肿。不幸的是,到入院第39天,患者感染持续进展,最终死于感染性休克。
诺卡菌性脑脓肿死亡率较高,尤其是在免疫功能低下患者和多发性脓肿患者中。及时诊断、积极的手术干预和敏感的抗生素治疗为治愈诺卡菌病提供了最佳前景。结核性脑膜炎是结核分枝杆菌感染最致命的表现形式,往往主要由于诊断和治疗延迟而导致严重后果。GeneXpert/RIF检测作为一种新兴的诊断工具,为检测TBM提供了更敏感、快速的方法。对于临床高度怀疑TBM的患者,应立即开始经验性抗结核治疗。及时准确的管理以及持续监测患者病情对于获得良好预后至关重要。
不适用。