Department of Laboratory Medicine, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China.
Medicine (Baltimore). 2021 Jan 8;100(1):e24245. doi: 10.1097/MD.0000000000024245.
Myasthenia gravis (MG) is an autoimmune disorder of the neuromuscular junctions that leads to fluctuating weakness and disabling fatigability. Due to difficulty in breathing caused by weakness of the respiratory muscles, patients with MG are more susceptible to pneumonia and other respiratory infections. As many patients with MG are given immunosuppressive therapy, this makes them more prone to infections. However, coinfection with 3 pathogens is very rare.
Here, we report the case of a 41-year-old gentleman with MG who was receiving long-term steroid therapy. He presented with a cough with pale brown expectoration that occurred without obvious inducement, severe pain in the scapula, as well as swelling and weakness of both legs. Despite undergoing treatment, but his symptoms did not improve, prompting two additional hospital admissions over a period of several months.
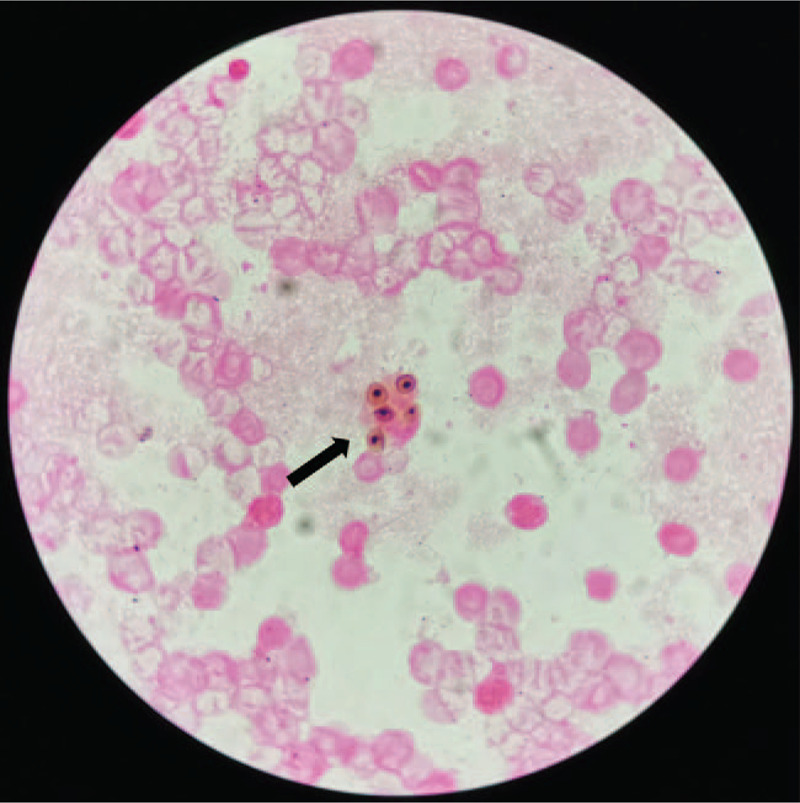
Bronchoscopy and bronchoalveolar lavage (BAL) were performed, revealing the presence of Pneumocystis jirovecii , Nocardia brasiliensis, and Mycobacterium tuberculosis (MTB). N brasiliensis was identified by positive modified acid-fast Kinyoun staining as well as a positive colony culture identified by matrix-assisted laser desorption ionization-time of flight mass spectrometry from the BAL sample. MTB was confirmed using GeneXpert, and due to the limitations of the culture conditions, methenamine silver stain was used to confirm Pneumocystis jirovecii. Next-generation sequencing (NGS) assay of the BAL samples also confirmed these pathogens.
The patient was transferred to a designated tuberculosis hospital and received anti-infective and anti-TB treatment.
During treatment at the designated hospital, the patient developed gastrointestinal bleeding and impaired liver function. One month later, he developed multiple organ failure, consolidation of the left lower lung, and pan-drug resistant bacteremia. He refused further treatment and was discharged.
In conclusion, physicians should be aware of the predisposition of MG patients to co-infections, especially patients with metabolic disorders, to avoid inadequate treatment and poor patient outcomes. Due to the limitations of culture conditions, NGS should be considered as a new technique for identifying pathogens.
重症肌无力(MG)是一种影响神经肌肉接头的自身免疫性疾病,可导致波动性无力和进行性疲劳。由于呼吸肌无力导致的呼吸问题,MG 患者更容易发生肺炎和其他呼吸道感染。由于许多 MG 患者接受免疫抑制治疗,因此他们更容易感染。然而,同时感染 3 种病原体非常罕见。
我们在此报告一例 41 岁男性 MG 患者,长期接受类固醇治疗。他因无明显诱因出现咳嗽,咳淡棕色痰,肩胛剧烈疼痛,双下肢肿胀、无力而就诊。尽管经过治疗,但症状仍未改善,在几个月的时间里,他又因同样的症状两次住院。
进行支气管镜检查和支气管肺泡灌洗(BAL),发现存在肺孢子菌、巴西奴卡菌和结核分枝杆菌(MTB)。BAL 样本经改良酸染色阳性和基质辅助激光解吸电离飞行时间质谱法鉴定的阳性菌落培养阳性,鉴定为巴西奴卡菌。MTB 经 GeneXpert 确认,由于培养条件的限制,使用六亚甲基四胺银染色确认肺孢子菌。BAL 样本的下一代测序(NGS)检测也证实了这些病原体的存在。
患者转至结核病定点医院,接受抗感染和抗结核治疗。
在定点医院治疗期间,患者出现胃肠道出血和肝功能损害。1 个月后,他出现多器官功能衰竭、左下肺实变和泛耐药菌血症。他拒绝进一步治疗并出院。
总之,医生应意识到 MG 患者易合并感染,尤其是代谢紊乱患者,以避免治疗不足和患者预后不良。由于培养条件的限制,应考虑 NGS 作为一种新的病原体鉴定技术。