Kea Bory, Warton E Margaret, Kutz Candice E, Kinney Erin, Ballard Dustin W, Reed Mary E, Lip Gregory Y H, Raitt Merritt, Sun Benjamin C, Vinson David R
Department of Emergency Medicine, Oregon Health and Science University, Portland, OR, USA.
School of Medicine, Oregon Health and Science University, Portland, OR, USA.
Int J Emerg Med. 2025 May 13;18(1):97. doi: 10.1186/s12245-025-00887-3.
Oral anticoagulation (OAC) reduces stroke and mortality risk in patients with non-valvular atrial fibrillation/flutter (AF). Patterns of OAC initiation upon discharge from US emergency departments (ED) are poorly understood. We sought to examine stroke prophylaxis actions upon, and shortly following, ED discharge of stroke-prone AF patients.
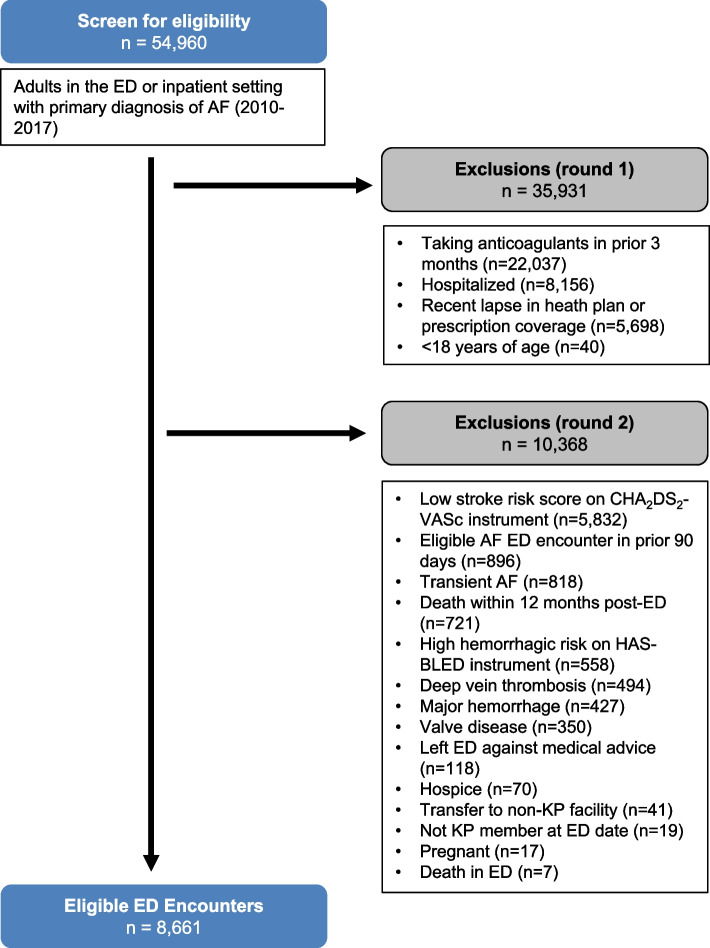
We included all adults with a primary diagnosis of non-valvular AF, high stroke risk (CHADS-VASc ≥ 2), low/intermediate bleeding risk (HAS-BLED < 4), and no recent (< 90 days) OAC at discharge from 21 community EDs (2010-2017). Annual rates of appropriate stroke prevention action (OAC Action) were calculated for eligible discharges and as defined as an OAC prescription or anticoagulation management service consultation within 14 days of ED discharge. We modeled OAC Action using a parsimonious Poisson regression with identity link adjusting for sex, age, race/ethnicity, stroke risk score (CHADS-VASc), year of visit, provider race/ethnicity, number of ED beds, and presence of an outpatient observation unit, with the patient as a random effect.
We studied 9,603 eligible ED discharges (mean age 73.1 ± 11.4 years, 62.3% female), and mean CHADS-VASc score 3.5 ± 1.5. From 2010 to 2017, OAC Action increased from 21.0% to 33.5%. Factors associated with lower OAC initiation included the following: female sex (-3.6%, 95% CI -5.4 to -1.9), age ≥ 85 vs < 64 years (-3.8%, 95% CI -6.7 to -1.0%), ED beds, n = 20 to 29 (-5.3%, 95% CI -8.36 to -2.4%), 30-49 (-3.8, 95% CI -6.5 to -1.2%), and 50 + (-7.1%, 95% CI -10.6 to -3.7%); with referent being the male sex, < 40 years, and fewer than 20 beds (18.1%, 95% CI 12.8 to 23.4). OAC initiation in 2017 was greater than in 2010 (16.0%, 95% CI 12.3 to 19.7%).
Within a community-based ED population of AF patients at high stroke risk, rates of appropriate stroke prevention action increased over the 7-year study period. Rates of AF thromboprophylaxis may be improved by addressing sex and age disparities, as females and those age ≥ 75 were less likely to receive indicated stroke prevention.
口服抗凝治疗(OAC)可降低非瓣膜性心房颤动/心房扑动(AF)患者的中风和死亡风险。美国急诊科(ED)出院时OAC起始治疗的模式尚不清楚。我们试图研究易中风AF患者在ED出院时及出院后不久的中风预防措施。
我们纳入了2010年至2017年期间从21个社区急诊科出院的所有主要诊断为非瓣膜性AF、中风风险高(CHADS-VASc≥2)、出血风险低/中度(HAS-BLED<4)且近期(<90天)未接受OAC治疗的成年人。计算符合条件出院患者的适当中风预防措施(OAC措施)的年发生率,定义为ED出院后14天内开具OAC处方或进行抗凝管理服务咨询。我们使用简约泊松回归模型对OAC措施进行建模,采用恒等连接函数,对性别、年龄、种族/民族、中风风险评分(CHADS-VASc)、就诊年份、医疗服务提供者种族/民族、ED病床数量以及是否设有门诊观察单元进行调整,并将患者作为随机效应。
我们研究了9603例符合条件的ED出院患者(平均年龄73.1±11.4岁,62.3%为女性),平均CHADS-VASc评分为3.5±1.5。从2010年到2017年,OAC措施从21.0%增加到33.5%。与OAC起始治疗率较低相关的因素包括:女性(-3.6%,95%CI为-5.4至-1.9)、年龄≥85岁与<64岁相比(-3.8%,95%CI为-6.7至-1.0%)、ED病床数量为20至29张(-5.3%,95%CI为-8.36至-2.4%)、30至49张(-3.8,95%CI为-6.5至-1.2%)以及50张及以上(-7.1%,95%CI为-10.6至-3.7%);以男性、<40岁且病床少于20张为参照组(18.1%,95%CI为12.8至23.4%)。2017年的OAC起始治疗率高于2010年(16.0%,95%CI为12.3至19.7%)。
在以社区为基础的高中风风险AF患者的ED人群中,在7年的研究期间,适当中风预防措施的发生率有所增加。通过解决性别和年龄差异问题,AF血栓预防率可能会得到提高,因为女性和年龄≥75岁的患者接受指定中风预防治疗的可能性较小。