Busto Giorgio, Morotti Andrea, Casetta Ilaria, Poggesi Anna, Gadda Davide, Ginestroni Andrea, Arcara Giorgio, Rustici Arianna, Zini Andrea, Padovani Alessandro, Fainardi Enrico
Neuroradiology Unit, Department of Radiology, Careggi University Hospital, 50134 Florence, Italy.
Neurology Unit, Department of Clinical and Experimental Sciences, University of Brescia, 25121 Brescia, Italy.
J Clin Med. 2025 Apr 25;14(9):2991. doi: 10.3390/jcm14092991.
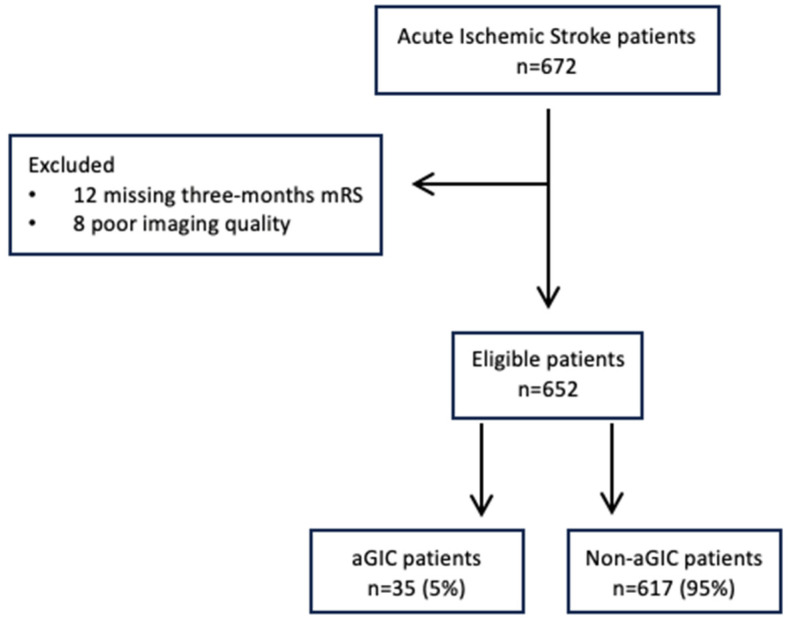
CT perfusion (CTP) overestimation of core volume >10 mL compared to the final infarct volume (FIV) size is the current definition of the ghost infarct core (GIC) phenomenon. However, subsequent infarct growth might influence FIV. We aimed to report a more reliable assessment of GIC occurrence, defined as no evidence of infarct at 24 h follow-up imaging, compared to CTP core volume at admission. This phenomenon was named absolute GIC (aGIC), and we investigated its prevalence and predictors. A total of 652 consecutive stroke patients with large vessel occlusion who achieved successful recanalization (mTICI 2b-3) after endovascular treatment (EVT) and non-contrast CT (NCCT) follow-up imaging at 24 h were retrospectively analyzed. Ischemic core volume was automatically generated from CTP, and FIV was manually determined on follow-up NCCT. Multivariable logistic regression was used to explore aGIC predictors. We included 652 patients (53.3% female, median age 75 years), of whom 35 (5.3%) had an aGIC. The aGIC group showed higher ASPECTS ( < 0.001), shorter (<3 h) onset-to-imaging time ( < 0.016), poorer collaterals ( < 0.001), and higher hypoperfusion intensity ratio ( < 0.001) compared to the non-aGIC group. In multivariate analysis, ASPECTS (odds ratio (OR), 2.37; <0.001), onset-to-imaging time (OR, 0.99; = 0.034), collateral score (OR, 0.24; < 0.001), and hypoperfusion intensity ratio (OR, 23.2; < 0.001) were independently associated with aGIC. aGIC is a more reliable evaluation of infarct core volume overestimation assessed on admission CTP and represents a rare phenomenon, associated with ultra-early presentation and poor collaterals.
与最终梗死体积(FIV)相比,CT灌注(CTP)高估核心体积>10 mL是目前幽灵梗死核心(GIC)现象的定义。然而,随后的梗死灶扩大可能会影响FIV。我们旨在报告一种更可靠的GIC发生率评估方法,其定义为在24小时随访成像时无梗死证据,与入院时CTP核心体积相比。这种现象被命名为绝对GIC(aGIC),我们调查了其患病率和预测因素。对652例接受血管内治疗(EVT)后成功再通(mTICI 2b - 3)且在24小时进行非增强CT(NCCT)随访成像的连续大动脉闭塞性卒中患者进行了回顾性分析。缺血核心体积由CTP自动生成,FIV在随访NCCT上手动确定。采用多变量逻辑回归来探索aGIC的预测因素。我们纳入了652例患者(53.3%为女性,中位年龄75岁),其中35例(5.3%)有aGIC。与非aGIC组相比,aGIC组的ASPECTS评分更高(<0.001),发病至成像时间更短(<3小时)(<0.016),侧支循环更差(<0.001),灌注不足强度比更高(<0.001)。在多变量分析中,ASPECTS评分(比值比(OR),2.37;<0.001)、发病至成像时间(OR,0.99;=0.034)、侧支循环评分(OR,0.24;<0.001)和灌注不足强度比(OR,23.2;<0.001)与aGIC独立相关。aGIC是对入院时CTP评估的梗死核心体积高估的更可靠评估,是一种罕见现象,与超早期表现和侧支循环差有关。