Jankowski Piotr, Topór-Mądry Roman, Kozieł Paweł, Cieśla Daniel, Cegłowska Urszula, Burzyńska Monika, Eysymontt Zbigniew, Sierpiński Radosław, Pinkas Jarosław, Gąsior Mariusz
Department of Internal Medicine and Geriatric Cardiology, Centre of Postgraduate Medical Education, 02-507 Warsaw, Poland.
Department of Epidemiology and Health Promotion, Centre of Postgraduate, School of Public Health, 01-826 Warsaw, Poland.
J Clin Med. 2025 Apr 26;14(9):3007. doi: 10.3390/jcm14093007.
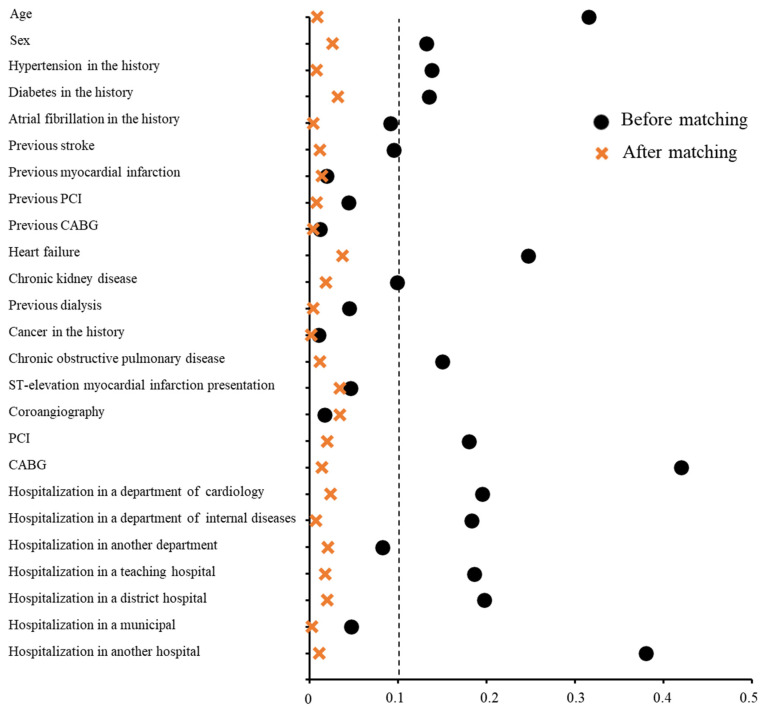
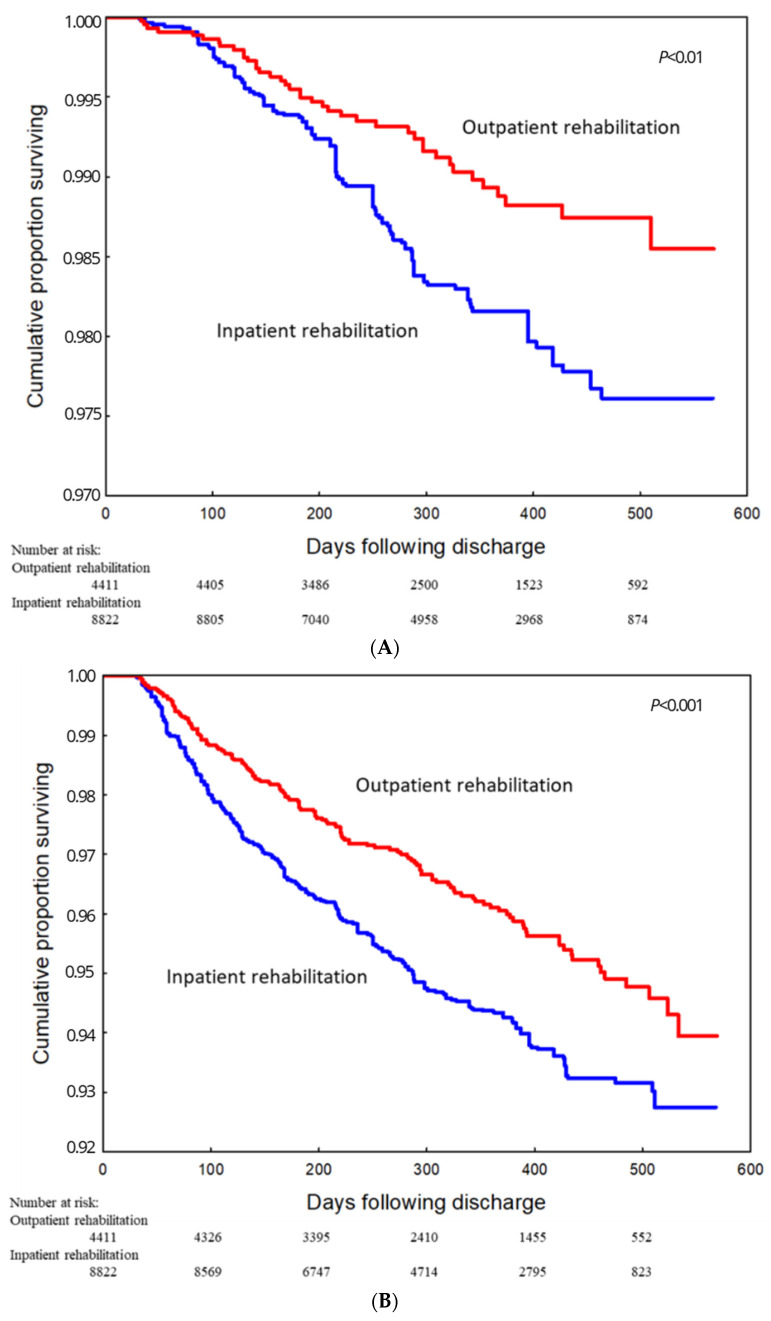
Models of second-phase cardiac rehabilitation (CR) following myocardial infarction (MI) differ across countries. The aim of this study was to compare outcomes in MI survivors participating in outpatient and inpatient CR programs. All patients hospitalized for acute MI in Poland between October 2017 and December 2018 (n = 96,634) were included in the study. Among them, 4411 patients were referred to and commenced outpatient CR, whereas 11,626 patients started inpatient CR within 30 days following discharge. The mean follow-up period was 332.8 ± 128.1 days. Younger age, male sex, and a history of cancer were associated with a higher probability of participating in outpatient CR, whereas diabetes, heart failure, chronic kidney disease, chronic obstructive pulmonary disease, ST-elevation MI, and myocardial revascularization were associated with a lower likelihood of outpatient CR participation. Participation in outpatient CR was linked to a reduced risk of all-cause mortality, in both univariable (hazard ratio [95% confidence interval]: 0.37 [0.26-0.51]) and multivariable analyses (0.53 [0.38-0.74]). Outpatient CR was also associated with a lower risk of death, MI, or stroke (0.57 [0.48-0.67] in univariable analysis and 0.72 [0.61-0.84] in multivariable analysis), as well as a lower risk of death or cardiovascular hospitalization (0.78 [0.73-0.84] and 0.85 [0.80-0.91], respectively). Outpatient CR following MI tends to occur alongside a better prognosis compared to inpatient programs.
心肌梗死后第二阶段心脏康复(CR)模式在不同国家存在差异。本研究的目的是比较参与门诊和住院CR项目的心肌梗死幸存者的结局。2017年10月至2018年12月期间在波兰因急性心肌梗死住院的所有患者(n = 96,634)均纳入本研究。其中,4411例患者被转诊并开始门诊CR,而11,626例患者在出院后30天内开始住院CR。平均随访期为332.8±128.1天。年龄较小、男性以及有癌症病史与参与门诊CR的较高概率相关,而糖尿病、心力衰竭、慢性肾病、慢性阻塞性肺疾病、ST段抬高型心肌梗死和心肌血运重建与参与门诊CR的较低可能性相关。参与门诊CR与全因死亡率降低相关,单变量分析(风险比[95%置信区间]:0.37[0.26 - 0.51])和多变量分析(0.53[0.38 - 0.74])均如此。门诊CR还与死亡、心肌梗死或中风风险降低相关(单变量分析中为0.57[0.48 - 0.67],多变量分析中为0.72[0.61 - 0.84]),以及死亡或心血管住院风险降低相关(分别为0.78[0.73 - 0.84]和0.85[0.80 - 0.91])。与住院项目相比,心肌梗死后的门诊CR往往伴随着更好的预后。