Wang Fanchang, Qiao Hongyang, Zheng Yi, Zheng Yating, Ni Yuxin, He Xiaoming
The Second Clinical Medical College of Zhejiang Chinese Medical University, Hangzhou, China.
The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China.
Front Public Health. 2025 May 1;13:1587194. doi: 10.3389/fpubh.2025.1587194. eCollection 2025.
The prevalence of obesity, a common metabolic disorder, has been increasing annually, particularly in older adults. This trend poses a significant socioeconomic burden. The uric acid to high-density lipoprotein cholesterol ratio (UHR) was defined by dividing UA (mg/dL) by HDL-C (mg/dL) and multiplying by 100%. According to recent clinical research, UHR has emerged as a potential innovative indicator in metabolic status evaluation, supported by contemporary biomarker research. This cross-sectional study investigated the association between the UHR index and obesity prevalence among older Americans.
This cross-sectional research employed nationally representative survey data to Examine the connection between the UHR index and obesity among older individuals aged 60 and above.
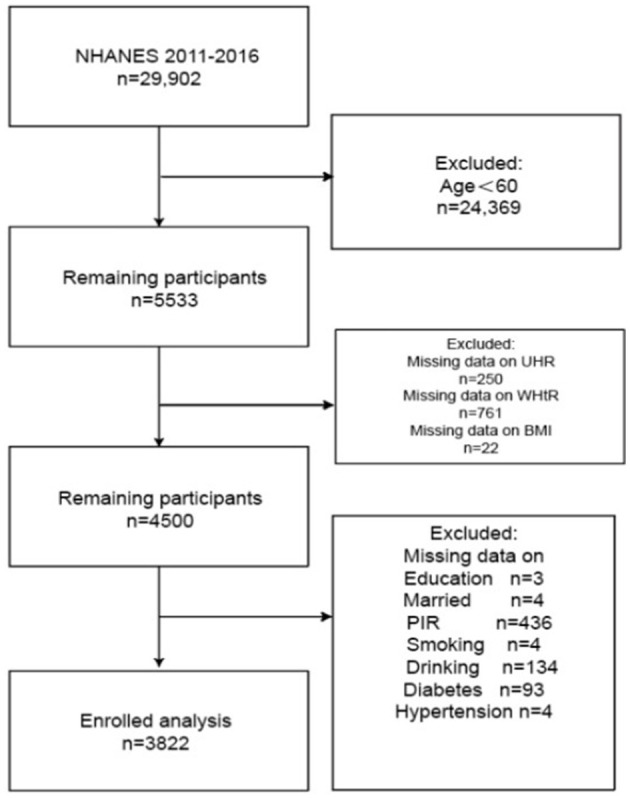
This study utilized data from the National Health and Nutrition Examination Survey (NHANES) spanning 2011 to 2016. Individuals who were 60 years old or older were included in the study ( = 3,822). The relationship between UHR levels and obesity (as measured by a body mass index of 30 kg/m or greater or a waist-to-height ratio (WHtR) ≥0.5) was investigated using weighted multivariable logistic regression analyses, with adjustments made for sociodemographic characteristics, behavioral patterns, and clinical covariates, adjusting for sociodemographic, behavioral, and clinical covariates. Restricted cubic spline, ROC curves, threshold analysis, and subgroup analysis were also used.
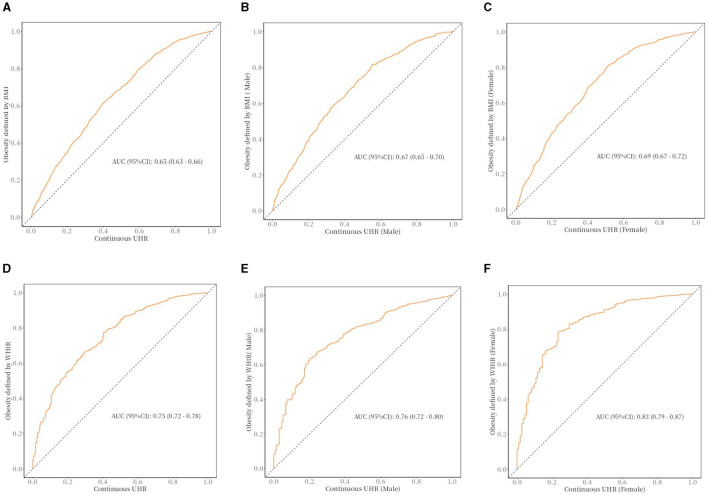
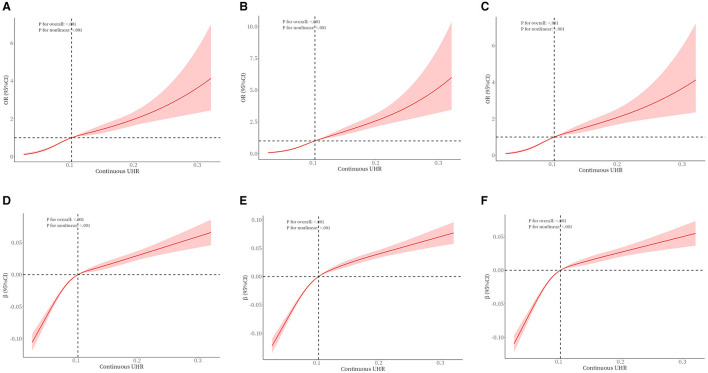
After full adjustment for confounders, UHR was positively associated with the risk of obesity as defined by BMI (highest quartile vs. lowest quartile: OR = 6.13, 95% CI = 4.01-9.39; -trend < 0.001) and UHR was positively associated with the risk of obesity as defined by WHtR (highest quartile vs. lowest quartile: OR = 20.21, 95% CI = 8.33-49.02; -trend < 0.001). In addition, The restricted cubic spline analysis uncovered a nonlinear dose-response relationship (P < 0.01), and threshold analysis found inflection points of -2.485 in obesity defined by BMI and -2.503 in WHtR. Subgroup analyses showed that the association between UHR and obesity in older Americans was consistent across subgroups, demonstrating high reliability (all P-interaction > 0.05). The AUC for UHR predicting obesity defined by BMI was calculated to be 0.65 (95% CI = 0.63-0.66). The UHR predicted AUC for obesity as defined by men's body mass index (BMI) was 0.67 (95% CI = 0.65-0.70). UHR predicted an AUC of 0.69 (95% CI = 0.67-0.72) for obesity defined by body mass index (BMI) in females. The AUC for UHR predicting obesity defined by WHtR was calculated to be 0.75 (95% CI = 0.72-0.78). UHR predicted an AUC of 0.76 (95% CI = 0.72-0.80) for obesity defined by WHtR in males, and UHR predicted an AUC of 0.83 (95% CI = 0.79-0.87) for obesity defined by WHtR in females.
The findings demonstrate a notable positive correlation between UHR and obesity in older adults, with this association remaining evident following adjustment for multiple confounding variables. These results imply that systematic evaluation of UHR levels could serve as an effective strategy for proactively detecting populations susceptible to obesity-related metabolic disorders.
肥胖是一种常见的代谢紊乱疾病,其患病率逐年上升,在老年人中尤为明显。这一趋势带来了巨大的社会经济负担。尿酸与高密度脂蛋白胆固醇比值(UHR)的定义为尿酸(mg/dL)除以高密度脂蛋白胆固醇(mg/dL)再乘以100%。根据最近的临床研究,在当代生物标志物研究的支持下,UHR已成为代谢状态评估中一个潜在的创新指标。这项横断面研究调查了美国老年人中UHR指数与肥胖患病率之间的关联。
这项横断面研究采用具有全国代表性的调查数据,以检验60岁及以上老年人中UHR指数与肥胖之间的联系。
本研究利用了2011年至2016年国家健康与营养检查调查(NHANES)的数据。纳入研究的对象为60岁及以上的个体(n = 3822)。使用加权多变量逻辑回归分析研究UHR水平与肥胖(以体重指数30 kg/m²或更高或腰高比(WHtR)≥0.5衡量)之间的关系,并对社会人口学特征、行为模式和临床协变量进行调整。还使用了受限立方样条、ROC曲线、阈值分析和亚组分析。
在对混杂因素进行全面调整后,UHR与体重指数定义的肥胖风险呈正相关(最高四分位数与最低四分位数相比:OR = 6.13,95%CI = 4.01 - 9.39;P趋势 < 0.001),UHR与腰高比定义的肥胖风险呈正相关(最高四分位数与最低四分位数相比:OR = 20.21,95%CI = 8.33 - 49.02;P趋势 < 0.001)。此外,受限立方样条分析发现了非线性剂量反应关系(P < 0.01),阈值分析发现体重指数定义的肥胖中的拐点为 -2.485,腰高比定义的肥胖中的拐点为 -2.503。亚组分析表明,美国老年人中UHR与肥胖之间的关联在各亚组中是一致的,显示出高度的可靠性(所有P交互作用 > 0.05)。UHR预测体重指数定义的肥胖的AUC计算为0.65(95%CI = 0.63 - 0.66)。UHR预测男性体重指数(BMI)定义的肥胖的AUC为0.67(95%CI = 0.65 - 0.70)。UHR预测女性体重指数(BMI)定义的肥胖的AUC为0.69(95%CI = 0.67 - 0.72)。UHR预测腰高比定义的肥胖的AUC计算为0.75(95%CI = 0.72 - 0.78)。UHR预测男性腰高比定义的肥胖的AUC为0.76(95%CI = 0.72 - 0.80),UHR预测女性腰高比定义的肥胖的AUC为0.83(95%CI = 0.79 - 0.87)。
研究结果表明老年人中UHR与肥胖之间存在显著的正相关,在对多个混杂变量进行调整后这种关联仍然明显。这些结果意味着对UHR水平进行系统评估可以作为一种有效的策略,用于主动检测易患肥胖相关代谢紊乱的人群。