Yamada Takeshi, Aoki Yuto, Matsuda Akihisa, Yokoyama Yasuyuki, Takahashi Goro, Iwai Takuma, Shinji Seiichi, Sonoda Hiromichi, Uehara Kay, Yoshida Hiroshi
Department of Gastroenterological Surgery Nippon Medical School Tokyo Japan.
Ann Gastroenterol Surg. 2024 Dec 5;9(3):538-545. doi: 10.1002/ags3.12894. eCollection 2025 May.
Despite the prevalence of laparoscopic techniques in abdominal surgeries today, bowel obstruction remains a potentially serious complication. Small bowel strangulation (SBS), in particular, is a critical condition that can lead to patient mortality. However, the prognosis for SBS is favorable if surgery is performed before the onset of necrosis. Non-necrotic SBS is a reversible condition in which blood flow can be restored by relieving the strangulation. The purpose of this study was to identify sensitive and specific contrast-enhanced computed tomography (CT) findings that are useful for diagnosis of both non-necrotic and necrotic SBS.
We included patients diagnosed with SBS and simple bowel obstruction (SBO) who underwent contrast-enhanced CT followed by surgery from 2006 to 2023. Two gastrointestinal surgeons independently assessed the images retrospectively.
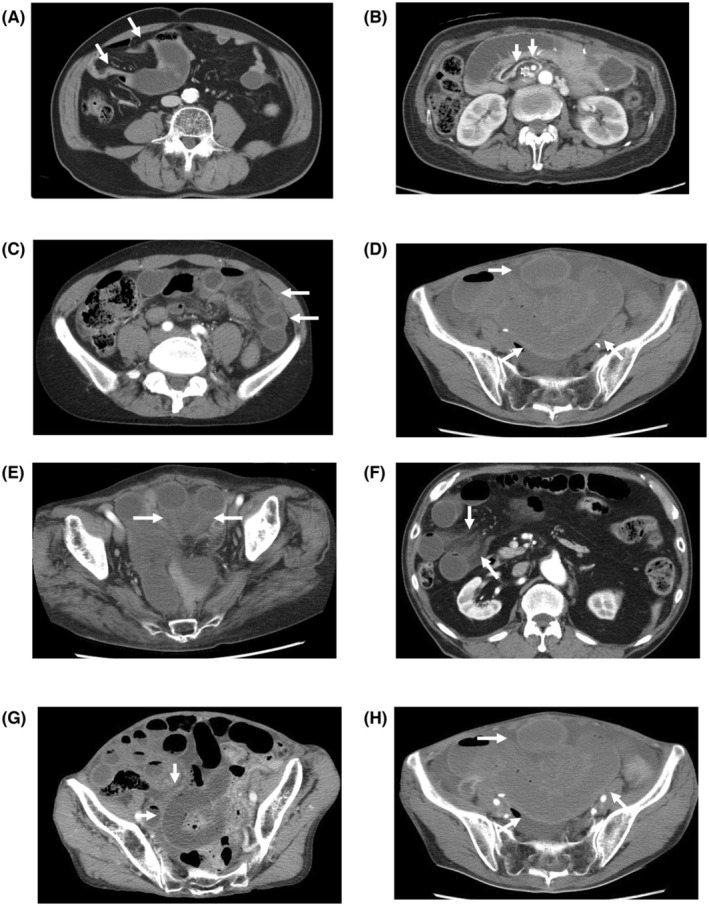
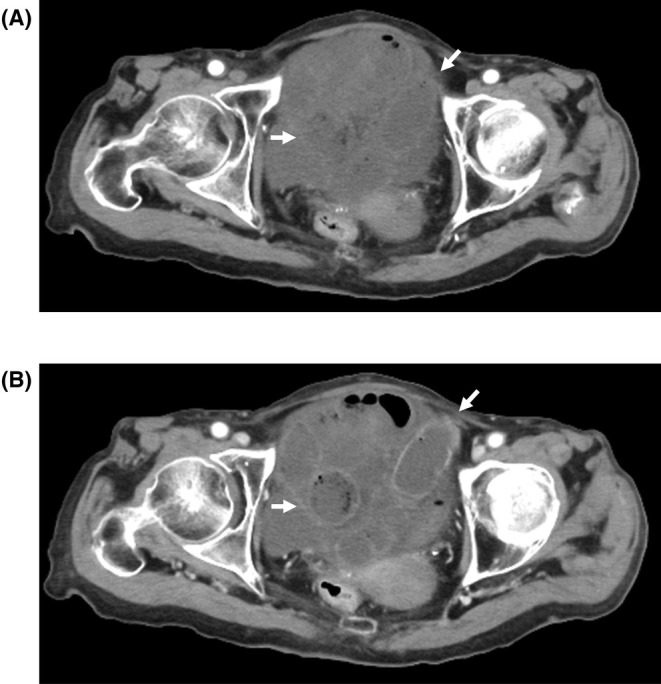
Eighty SBO and 141 SBS patients were included. Eighty-seven had non-necrotic SBS and 54 had necrotic SBS. Mesenteric edema was most frequently observed in both necrotic and non-necrotic SBS cases followed by abnormal bowel wall thickening. These two findings were observed significantly less frequently in SBO. Bowel hypo-enhancement is identified in only about half of the non-necrotic SBS cases, and it was detected at significantly higher rates in necrotic SBS compared to non-necrotic.
Mesenteric edema and abnormal bowel wall thickening are sensitive and specific signs of both non-necrotic and necrotic SBS. These two findings indicate mesenteric and bowel congestion. Detecting intestinal congestion can lead to an accurate diagnosis of SBS, particularly in case of non-necrotic SBS, where bowel hypo-enhancement may sometimes be absent.
尽管如今腹腔镜技术在腹部手术中广泛应用,但肠梗阻仍是一种潜在的严重并发症。特别是小肠绞窄(SBS),是一种可导致患者死亡的危急情况。然而,如果在坏死发生前进行手术,SBS的预后良好。非坏死性SBS是一种可逆性病症,通过解除绞窄可恢复血流。本研究的目的是确定敏感且特异的对比增强计算机断层扫描(CT)表现,以用于诊断非坏死性和坏死性SBS。
我们纳入了2006年至2023年间诊断为SBS和单纯性肠梗阻(SBO)并接受了对比增强CT检查及后续手术的患者。两名胃肠外科医生对图像进行了回顾性独立评估。
纳入了80例SBO患者和141例SBS患者。其中87例为非坏死性SBS,54例为坏死性SBS。肠系膜水肿在坏死性和非坏死性SBS病例中最常被观察到,其次是肠壁异常增厚。这两个表现在SBO中观察到的频率显著较低。肠壁强化减低仅在约一半的非坏死性SBS病例中被发现,与非坏死性SBS相比,在坏死性SBS中检测到的比例显著更高。
肠系膜水肿和肠壁异常增厚是诊断非坏死性和坏死性SBS敏感且特异的征象。这两个表现提示肠系膜和肠管充血。检测到肠管充血可准确诊断SBS,特别是在非坏死性SBS的情况下,有时可能不存在肠壁强化减低。