Wang Xinyu, Wang Yuming, Cao Min, Fu Yujie, Pan Wenbiao, Ye Qing, Zhao Xiaojing, Sun Zhiyong
Department of Thoracic Surgery, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200040, China.
Shanghai Chest Hospital, Shanghai Lung Cancer Center, Shanghai Jiao Tong University School of Medicine, Shanghai, 200040, China.
BMC Surg. 2025 May 21;25(1):220. doi: 10.1186/s12893-025-02944-3.
Resection of basal segmentectomy through uniportal video-assisted thoracoscopic surgery (U-VATS) is technically challenging for thoracic surgeons. Compared with multiportal VATS (M-VATS), the safety and feasibility of U-VATS for complex segmentectomy of lower lung lobe need further validation. In this study, we aimed to compare the perioperative outcomes of U-VATS with M-VATS in the treatment of complex segmentectomy of lower lung lobe for stage IA lung cancer.
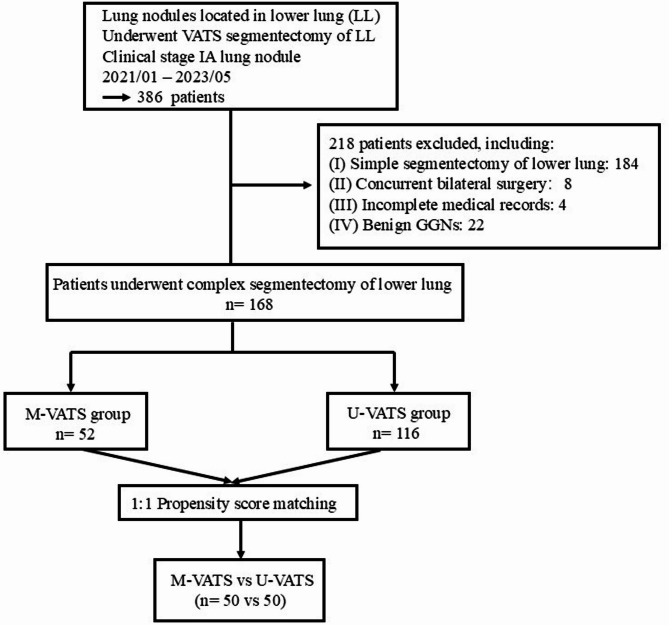
We conducted a retrospective cohort study of 168 patients (116 U-VATS and 52 M-VATS) undergoing complex lower lobe segmentectomy for stage IA NSCLC from January 2021 to May 2023. The demographics of the enrolled patients were collected and propensity score matching (PSM) was used to reduce the heterogeneity of baseline characteristics. Perioperative outcomes were compared between the two groups.
After matching, 50 cases were yielded in each group. There was no 30-day postoperative mortality and conversion to open in both groups. The U-VATS exhibited shorter postoperative hospital stays (P = 0.034) and a trend toward reduced postoperative drainage (P = 0.081) compared to the M-VATS group. Pain score on postoperative day 2 in the U-VATS group was lower than M-VATS group (P = 0.004). There were no significant differences in resection margins, operation time and postoperative complications between the two groups.
U-VATS provides comparable perioperative safety and efficacy to M-VATS for complex lower lobe segmentectomy, with advantages in accelerated recovery and reduced postoperative pain. U-VATS complex segmentectomy of lower lung lobe is a safe and feasible technique for experienced thoracic surgeons, which deserves support and popularity.
通过单孔电视辅助胸腔镜手术(U-VATS)进行基底段切除术对胸外科医生来说在技术上具有挑战性。与多孔电视辅助胸腔镜手术(M-VATS)相比,U-VATS用于下肺叶复杂节段切除术的安全性和可行性需要进一步验证。在本研究中,我们旨在比较U-VATS与M-VATS治疗IA期肺癌下肺叶复杂节段切除术的围手术期结果。
我们对2021年1月至2023年5月期间接受IA期非小细胞肺癌下叶复杂节段切除术的168例患者(116例U-VATS和52例M-VATS)进行了一项回顾性队列研究。收集纳入患者的人口统计学数据,并使用倾向评分匹配(PSM)来减少基线特征的异质性。比较两组的围手术期结果。
匹配后,每组产生50例。两组均无术后30天死亡率和中转开胸情况。与M-VATS组相比,U-VATS术后住院时间更短(P = 0.034),术后引流有减少趋势(P = 0.081)。U-VATS组术后第2天的疼痛评分低于M-VATS组(P = 0.004)。两组在切缘、手术时间和术后并发症方面无显著差异。
对于下肺叶复杂节段切除术,U-VATS与M-VATS具有相当的围手术期安全性和疗效,在加速康复和减轻术后疼痛方面具有优势。U-VATS下肺叶复杂节段切除术对于经验丰富的胸外科医生来说是一种安全可行的技术,值得支持和推广。