Wu Shixing, Li Jiangang, Zhang Bolin, Wang Cheng, Abuduwaili Atigu, Zhang Junxiang, Zhang Shouchao, Geng Cheng, Xu Xinjian
Department of Hepatobiliary and Pancreatic Surgery, The Fifth Affiliated Hospital of Xinjiang Medical University, Urumqi, PR China.
Sci Prog. 2025 Apr-Jun;108(2):368504251345016. doi: 10.1177/00368504251345016. Epub 2025 May 21.
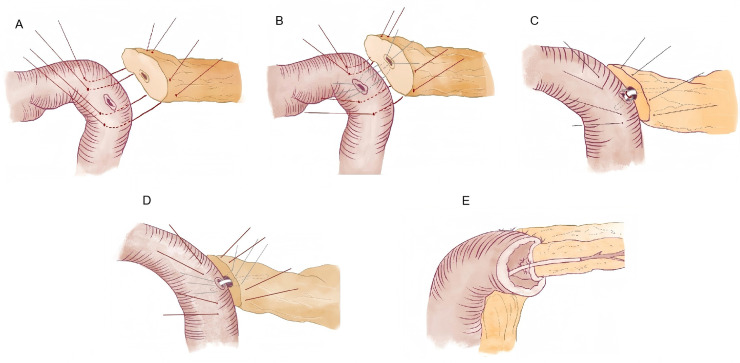
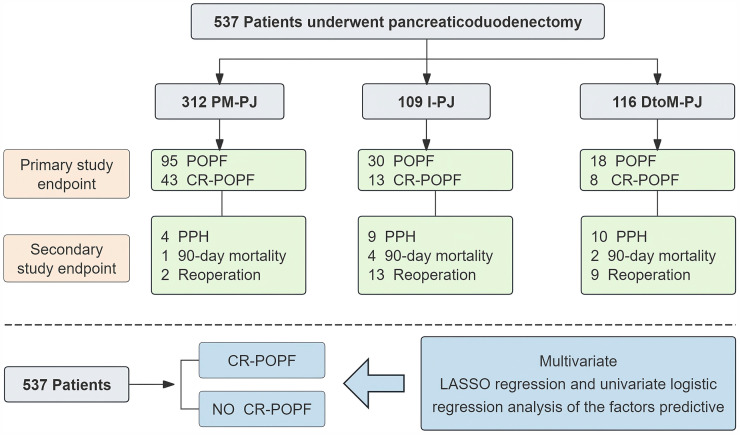
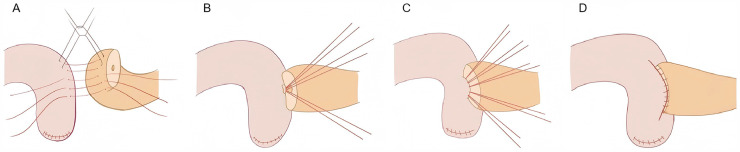
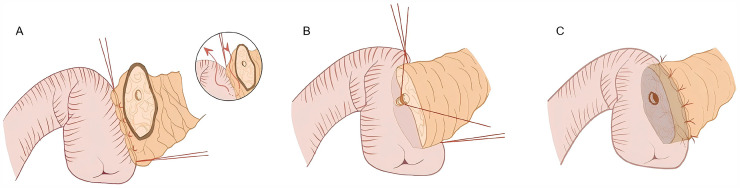
ObjectiveThe technological aspects of pancreaticoduodenectomy have progressed greatly, but the risk of postoperative complications, especially postoperative pancreatic fistula (POPF), postpancreatectomy haemorrhage (PPH) and mortality, is high. Therefore, we aimed to explore the safety and feasibility of pancreaticojejunostomy (PJ) under the mucosal priority healing theory through a case-control study.MethodsWe have described in detail PJ under the theory of preferential mucosal healing (PM-PJ). In a cohort of patients based on predictors of pancreatic fistula, comparisons were made according to the type of PJ: PM-PJ (n = 312); duct-to-mucosa PJ (DtoM-PJ, n = 116); and invagination PJ (IPJ, n = 109). The primary endpoint was the occurrence of clinically relevant postoperative pancreatic fistula (CR-POPF). The secondary endpoints were PPH, secondary surgery, death 90 days after surgery, and other postoperative complications.ResultsThe incidence rate of CR-POPF in the PM-PJ group was not significantly different from that in the DtoM-PJ group (13.78% vs. 6.9%; p = 0.051) or the IPJ group (13.78% vs. 11.9%; p = 0.623). However, the PM-PJ group exhibited significant reductions in serious postoperative complications (7.4% versus 30.2%; ), PPH (1.3% versus 8.4%; ), reoperation rates (0.6% versus 9.3%; ) and 90-day postoperative mortality rates (0.32% versus 2.6%; ). Multivariate LASSO regression analysis revealed that BMI, hypertension, gland texture, duct size, vascular resection and pathological type were independent risk factors for CR-POPF.ConclusionsPM-PJ is safe and reliable. During surgery, there are fewer suture needles and less trauma, which may reduce the incidence of serious complications such as postoperative bleeding and mortality.
目的
胰十二指肠切除术的技术层面已取得巨大进展,但术后并发症风险,尤其是术后胰瘘(POPF)、胰十二指肠切除术后出血(PPH)及死亡率仍很高。因此,我们旨在通过一项病例对照研究,探讨在黏膜优先愈合理论下胰空肠吻合术(PJ)的安全性和可行性。
方法
我们已详细描述了基于优先黏膜愈合理论的胰空肠吻合术(PM-PJ)。在一组基于胰瘘预测因素的患者中,根据PJ类型进行比较:PM-PJ(n = 312);导管对黏膜胰空肠吻合术(DtoM-PJ,n = 116);以及套入式胰空肠吻合术(IPJ,n = 109)。主要终点是临床相关术后胰瘘(CR-POPF)的发生情况。次要终点包括PPH、二次手术、术后90天死亡以及其他术后并发症。
结果
PM-PJ组CR-POPF的发生率与DtoM-PJ组(13.78%对6.9%;p = 0.051)或IPJ组(13.78%对11.9%;p = 0.623)相比无显著差异。然而,PM-PJ组在严重术后并发症(7.4%对30.2%; )、PPH(1.3%对8.4%; )、再次手术率(0.6%对9.3%; )及术后90天死亡率(0.32%对2.6%; )方面均有显著降低。多变量LASSO回归分析显示,BMI、高血压、腺体质地、导管大小、血管切除及病理类型是CR-POPF的独立危险因素。
结论
PM-PJ安全可靠。手术过程中,缝合针较少且创伤较小,这可能降低术后出血和死亡率等严重并发症的发生率。