Zheng Jingmao, Zhu Zhipeng, Xie Zhaolin, Cheng Zhilin, Chen Tianpei, Wu Qinmian, Li Ying
Department of Orthopedics, Guigang City People's Hospital, The Eighth Affiliated Hospital of Guangxi Medical University, Guigang City, China.
Medicine (Baltimore). 2025 May 23;104(21):e42479. doi: 10.1097/MD.0000000000042479.
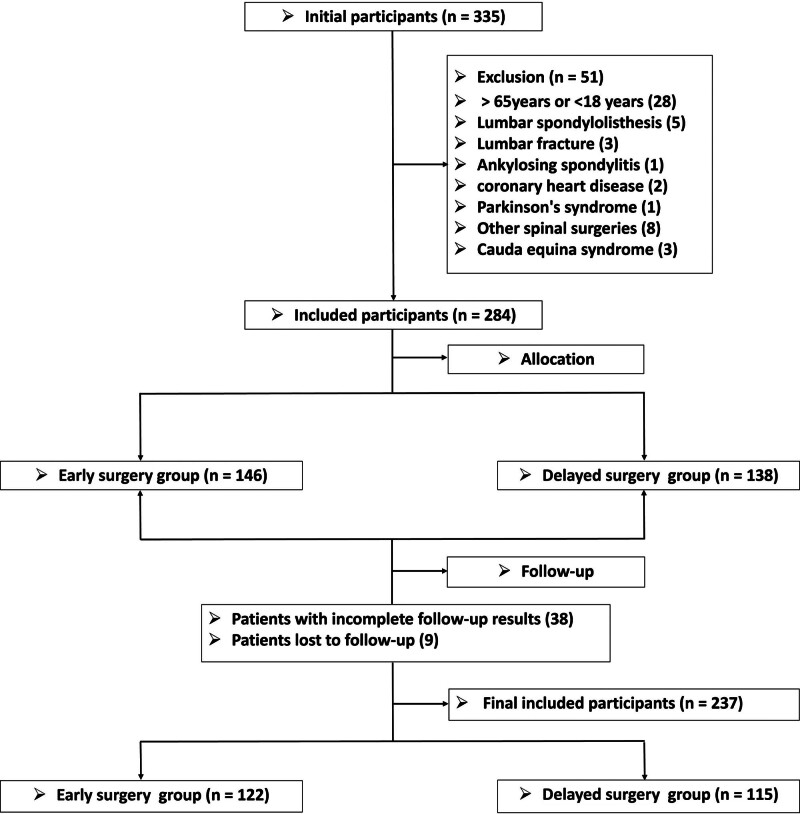
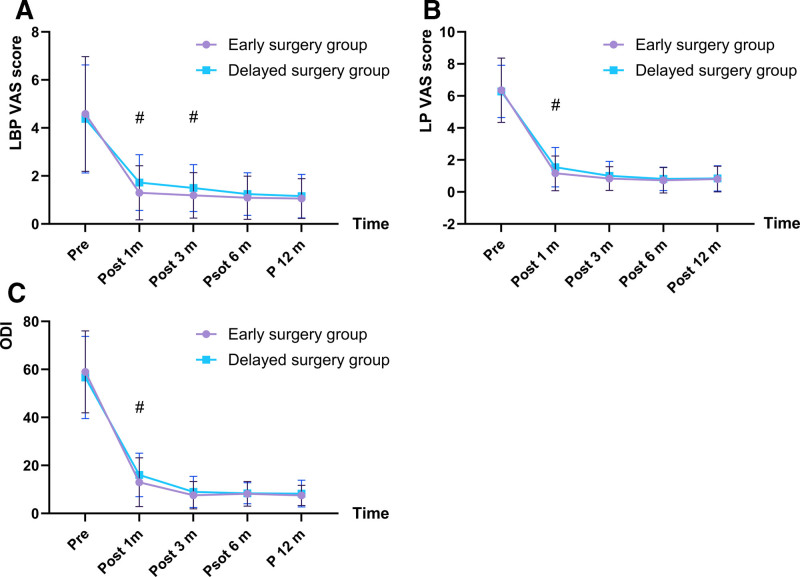
Lumbar discectomy can improve symptoms of sciatica caused by lumbar disc herniation (LDH) faster than conservative treatment. However, the optimal timing of surgery for LDH has scarcely been explored. The prospectively collected clinical outcome data from patients who underwent microdiscectomy for sciatica due to LDH were retrospectively analyzed. Patients were divided into 2 groups according to the duration of sciatica before surgery: early surgery (<6 months); and delayed surgery (≥6 months). Visual analog scale (VAS) scores for low back pain (LBP), leg pain (LP), and Oswestry disability index (ODI) were compared between the 2 groups preoperatively, and at 1, 3, 6, and 12 months postoperatively. In total, 122 and 115 patients comprised the early and delayed surgery groups, respectively. There were no significant differences between the 2 groups in terms of sex, age, body mass index, comorbidities, surgical procedure, surgical segment, preoperative LBP, LP VAS scores, or ODI. A significantly higher proportion of patients in the delayed surgery group were prescribed opioids preoperatively versus those in the early surgery group (25.2% vs 10.7%, respectively; P = .003). The duration of sciatica was significantly shorter in the early surgery group than that in the delayed surgery group (3.9 vs 12.2 months; P < .001). LBP VAS scores were significantly lower in the early versus delayed surgery group at 1 and 3 months postoperatively. Additionally, LP VAS scores and ODI in the early surgery group were significantly lower than those in the delayed surgery group at 1 month postoperatively. There was no significant difference in complication rates between the 2 groups (5.7% vs 5.2%; P = .860). Compared with delayed surgery, early surgery improved pain and disability in patients diagnosed with sciatica. However, this advantage tended to decline over time postoperatively, resulting in comparable long-term outcomes.
腰椎间盘切除术改善腰椎间盘突出症(LDH)所致坐骨神经痛症状的速度比保守治疗更快。然而,LDH手术的最佳时机鲜有研究。对前瞻性收集的因LDH接受显微椎间盘切除术治疗坐骨神经痛患者的临床结局数据进行回顾性分析。根据术前坐骨神经痛持续时间将患者分为两组:早期手术组(<6个月);延迟手术组(≥6个月)。比较两组术前、术后1、3、6和12个月时的下腰痛(LBP)、腿痛(LP)视觉模拟量表(VAS)评分及Oswestry功能障碍指数(ODI)。早期手术组和延迟手术组分别有122例和115例患者。两组在性别、年龄、体重指数、合并症、手术方式、手术节段、术前LBP、LP VAS评分或ODI方面无显著差异。延迟手术组术前使用阿片类药物的患者比例显著高于早期手术组(分别为25.2%和10.7%;P = 0.003)。早期手术组坐骨神经痛持续时间显著短于延迟手术组(3.9个月对12.2个月;P < 0.001)。术后1个月和3个月时,早期手术组的LBP VAS评分显著低于延迟手术组。此外,术后1个月时,早期手术组的LP VAS评分和ODI显著低于延迟手术组。两组并发症发生率无显著差异(5.7%对5.2%;P = 0.860)。与延迟手术相比,早期手术改善了坐骨神经痛患者的疼痛和功能障碍。然而,这种优势在术后随时间推移趋于下降,导致长期结局相当。