Jenkins Emily N, Gold Jeremy A W, Benedict Kaitlin, Lockhart Shawn R, Berkow Elizabeth L, Dixon Tamia, Shack Shanita L, Witt Lucy S, Harrison Lee H, Seopaul Shannon, Correa Maria A, Fitzsimons Megan, Jabarkhyl Yalda, Barter Devra, Czaja Christopher A, Johnston Helen, Markus Tiffanie, Schaffner William, Gross Annastasia, Lynfield Ruth, Tourdot Laura, Nadle Joelle, Roland Jeremy, Escutia Gabriela, Zhang Alexia Y, Gellert Anita, Hurley Christine, Tesini Brenda L, Phipps Erin C, Davis Sarah Shrum, Lyman Meghan
MMWR Surveill Summ. 2025 May 29;74(4):1-15. doi: 10.15585/mmwr.ss7404a1.
PROBLEM/CONDITION: Candidemia, a bloodstream infection caused by Candida spp., is a common cause of health care-associated bloodstream infections in the United States. Candidemia is associated with substantial health care costs, morbidity, and mortality.
2017-2021.
CDC's Emerging Infections Program (EIP), a collaboration among CDC, state health departments, and academic partners, was used to conduct active, population-based laboratory surveillance for candidemia at city or county sites located in 10 states (California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee), representing a combined population of approximately 21.5 million persons, or 7% of the U.S. population in 2019. Connecticut began reporting cases on January 1, 2019, and conducts statewide surveillance. Although candidemia is not a nationally notifiable condition, cases of Candida auris infection are nationally notifiable, and cases of candidemia caused by C. auris could be included in both national case counts and EIP surveillance. A culture-confirmed candidemia case is defined as a positive blood culture for any Candida sp. from a resident in the surveillance catchment area. Subsequent positive blood cultures for Candida within 30 days of the initial positive culture (index date) in the same patient are considered part of the same case. Clinical laboratories serving each catchment area report candidemia cases, and trained surveillance officers abstract information from medical charts for all cases. Corresponding isolates are sent to CDC for species confirmation and antifungal susceptibility testing.
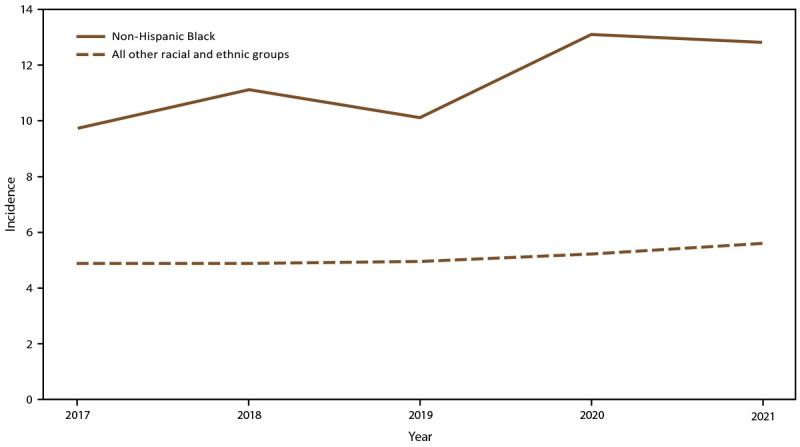
A total of 7,381 candidemia cases were identified during the surveillance period (2017-2021). The overall incidence was 7.4 cases per 100,000 population. Across age groups, sexes, racial and ethnic groups, and surveillance sites, incidence was generally stable or increased slightly from 2017 to 2021, with the lowest overall incidence in 2019 (6.8) and the highest in 2021 (7.9). In 2021, candidemia incidence was highest in patients aged ≥65 years (22.7) and infants (aged <1 year) (8.0). Incidence was higher in males (8.7) compared with females (7.0) and higher in non-Hispanic Black or African American (Black) patients (12.8) compared with non-Black patients (5.6). Incidence was highest in Maryland (14.5), followed by Tennessee (10.1) and Georgia (10.0); incidence was lowest in Oregon (4.8). Increases occurred in the percentage of cases classified as health care onset (52.2% in 2017 to 58.0% in 2021). Overall, among 7,381 cases (in 6,235 patients), 63.7% occurred in patients who had a central venous catheter, 80.7% involved recent systemic antibiotic receipt, and 9.0% occurred in patients who had a history of injection drug use. The percentage of cases with a positive SARS-CoV-2 test during the 90 days before or after the index date increased from 10.4% in 2020 to 17.7% in 2021. From 2017 to 2021, the percentage of cases involving an intensive care unit stay before the index date increased from 38.3% to 44.9%. Echinocandins (e.g., micafungin) were used as treatment in 49.8% of cases, and azoles were used in 47.7%. The all-cause in-hospital mortality rate was 32.6%; this increased from 26.8% in 2019 to 36.1% in 2021. Overall, Candida albicans accounted for 37.1% of cases, followed by Candida glabrata (30.4%) and Candida parapsilosis (13.5%); however, C. glabrata was the most frequent species in California (38.4%) and Maryland (32.9%). Candida auris infections accounted for 0.4% of cases. Among 6,576 Candida isolates for which interpretive breakpoints exist and isolates were available for testing, 5.6% were fluconazole resistant, and <1% were echinocandin resistant. Antifungal resistance was stable for all antifungals tested across years.
Candidemia remains an important health care-associated infection. The disproportionate incidence among older adults, males, and Black patients is consistent with previous reports, and the overall incidence of candidemia has not changed substantially compared with previous EIP findings based on data collected during 2012-2016 (8.7 per 100,000 population). The higher mortality rate associated with candidemia during 2020-2021 likely reflects consequences of the COVID-19 pandemic, including strained health care systems and an increased population of patients who were susceptible to candidemia because of COVID-19-related critical illness.
Strict implementation of measures to prevent health care-associated bloodstream infections is important to help prevent candidemia cases. Health care officials and providers should be vigilant for candidemia as a complication of critical illness. Continued surveillance is needed to monitor for emerging populations at risk for candidemia and changes in antifungal resistance patterns, which can help guide antifungal treatment selection.
问题/状况:念珠菌血症是一种由念珠菌属引起的血流感染,是美国医疗保健相关血流感染的常见原因。念珠菌血症与高昂的医疗保健成本、发病率和死亡率相关。
2017 - 2021年。
美国疾病控制与预防中心(CDC)的新兴感染项目(EIP)是CDC、州卫生部门和学术合作伙伴之间的合作项目,用于在位于10个州(加利福尼亚州、科罗拉多州、康涅狄格州、佐治亚州、马里兰州、明尼苏达州、新墨西哥州、纽约州、俄勒冈州和田纳西州)的市县地区开展基于人群的念珠菌血症主动实验室监测,这些地区的总人口约为2150万,占2019年美国人口的7%。康涅狄格州于2019年1月1日开始报告病例,并进行全州范围的监测。尽管念珠菌血症并非全国法定报告疾病,但耳念珠菌感染病例是全国法定报告疾病,由耳念珠菌引起的念珠菌血症病例可能会被纳入全国病例计数和EIP监测。经培养确诊的念珠菌血症病例定义为来自监测集水区居民的任何念珠菌属血培养阳性。同一患者在初始阳性培养(索引日期)后30天内后续的念珠菌血培养阳性被视为同一病例的一部分。为每个集水区服务的临床实验室报告念珠菌血症病例,经过培训的监测人员从所有病例的病历中提取信息。相应的分离株被送往CDC进行菌种鉴定和抗真菌药敏试验。
在监测期间(2017 - 2021年)共识别出7381例念珠菌血症病例。总体发病率为每10万人7.4例。在各个年龄组、性别、种族和民族以及监测地点中,发病率从2017年到2021年总体上保持稳定或略有上升,2019年总体发病率最低(6.8),2021年最高(7.9)。2021年,≥65岁患者(22.7)和婴儿(<1岁)(8.0)的念珠菌血症发病率最高。男性(8.7)的发病率高于女性(7.0),非西班牙裔黑人或非裔美国人(黑人)患者(12.8)的发病率高于非黑人患者(5.6)。马里兰州的发病率最高(14.5),其次是田纳西州(10.1)和佐治亚州(10.0);俄勒冈州的发病率最低(4.8)。归类为医疗保健相关发病的病例百分比有所增加(从2017年的52.2%增至2021年的58.0%)。总体而言,在7381例病例(涉及6235名患者)中,63.7%发生在有中心静脉导管的患者中,80.7%涉及近期全身性抗生素使用,9.0%发生在有注射吸毒史的患者中。在索引日期之前或之后90天内SARS-CoV-2检测呈阳性的病例百分比从2020年的10.4%增至2021年的17.7%。从2017年到2021年,索引日期之前入住重症监护病房的病例百分比从38.3%增至44.9%。49.8%的病例使用棘白菌素(如米卡芬净)进行治疗,47.7%的病例使用唑类药物。全因院内死亡率为32.6%;这一比例从2019年的26.8%增至2021年的36.1%。总体而言,白色念珠菌占病例的37.1%,其次是光滑念珠菌(30.4%)和近平滑念珠菌(13.5%);然而,光滑念珠菌是加利福尼亚州(38.4%)和马里兰州(32.9%)最常见的菌种。耳念珠菌感染占病例的0.4%。在6576株有解释性断点且可用于检测的念珠菌分离株中,5.6%对氟康唑耐药,<1%对棘白菌素耐药。多年来,所有检测的抗真菌药物的耐药性保持稳定。
念珠菌血症仍然是一种重要的医疗保健相关感染。老年人、男性和黑人患者中发病率不成比例与先前报告一致,与基于2012 - 2016年收集的数据得出的EIP先前研究结果相比,念珠菌血症的总体发病率没有实质性变化(每10万人8.7例)。2020 - 2021年与念珠菌血症相关的较高死亡率可能反映了2019冠状病毒病(COVID - 19)大流行的影响,包括紧张的医疗保健系统以及因COVID - 19相关危重病而易患念珠菌血症的患者人数增加。
严格实施预防医疗保健相关血流感染的措施对于预防念珠菌血症病例很重要。卫生保健官员和提供者应警惕念珠菌血症作为危重病并发症的情况。需要持续监测以监测念珠菌血症的新出现的高危人群以及抗真菌耐药模式的变化,这有助于指导抗真菌治疗的选择。