Naftali Ben Haim Liron, Yehezkeli Veronika, Kratz Assaf, Dar Nimrod, Sharon Tal, Harel Gal, Burganski-Eliash Zvia, Belkin Avner
Meir Medical Center, Kfar Saba 4428164, Israel.
The Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv 39040, Israel.
Diagnostics (Basel). 2025 May 13;15(10):1226. doi: 10.3390/diagnostics15101226.
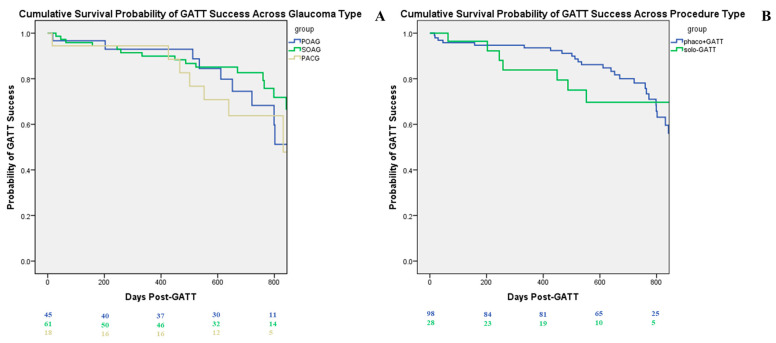
Gonioscopy-assisted transluminal trabeculotomy (GATT) is a minimally invasive, ab interno conjunctival-sparing glaucoma surgery aimed at the trabecular meshwork and the inner wall of Schlemm's canal. The goal of this study is to report on the success of GATT in a large group of patients with a wide variety of open- and closed-angle glaucomas with or without cataract extraction and to report on risk factors for failure. A retrospective chart review of consecutive patients with primary or secondary open- or closed-angle glaucoma who underwent GATT, with or without concomitant phacoemulsification. Demographics, baseline clinical characteristics, and postoperative outcomes were collected from patients' medical records. Primary outcomes were success rates (IOP of 18 mmHg or lower and one of the following: IOP reduction > 30% from baseline on the same or fewer medications or an IOP ≤ baseline with fewer medications as compared to baseline) and complication rates. Intraocular pressure (IOP) and the number of glaucoma medications were secondary outcome measures. GATT was performed on 126 eyes of 121 patients. Mean follow-up was 583 ± 266 days. Cumulative success at 1Y was 0.88 for GATT combined with cataract extraction, 0.96 for GATT alone, 0.88 for primary open-angle glaucoma (POAG), 0.89 for secondary open-angle glaucoma (SOAG), and 0.76 for primary angle-closure glaucoma (PACG). IOP decreased from a mean of 20.65 mmHg to 14.1 mmHg, and medication decreased from a mean of 3.47 to 1.4 at the last follow-up. Forty-four eyes (34%) were classified as failures. Factors associated with an increased risk of failure were worse preoperative corrected visual acuity (OR = 2.46, = 0.024) and a postoperative IOP spike (OR = 2.62, = 0.028). Twelve eyes (9.5%) required further surgery for IOP control. Risk factors for requiring further surgery for IOP control were preoperative maximal IOP (OR = 1.066, = 0.047) and a postoperative IOP spike (OR = 4.531, = 0.036). GATT achieved good surgical success with good IOP and medication reduction across a wide range of glaucomas, in combination with lens extraction or as a standalone procedure. GATT should be considered early in the treatment paradigm of medically uncontrolled glaucoma.
房角镜辅助经腔小梁切开术(GATT)是一种微创、经结膜内保留结膜的青光眼手术,目标是小梁网和施莱姆管内壁。本研究的目的是报告GATT在一大组患有各种开角型和闭角型青光眼且有或无白内障摘除的患者中的成功率,并报告失败的危险因素。对连续接受GATT(有或无同期超声乳化术)的原发性或继发性开角型或闭角型青光眼患者进行回顾性病历审查。从患者的病历中收集人口统计学、基线临床特征和术后结果。主要结局是成功率(眼压≤18 mmHg且符合以下之一:在使用相同或更少药物的情况下眼压较基线降低>30%,或与基线相比使用更少药物时眼压≤基线)和并发症发生率。眼压(IOP)和青光眼药物数量是次要结局指标。对121例患者的126只眼进行了GATT手术。平均随访时间为583±266天。GATT联合白内障摘除术1年时的累积成功率为0.88,单纯GATT为0.96,原发性开角型青光眼(POAG)为0.88,继发性开角型青光眼(SOAG)为0.89,原发性闭角型青光眼(PACG)为0.76。在最后一次随访时,眼压从平均20.65 mmHg降至14.1 mmHg,药物数量从平均3.47种降至1.4种。44只眼(34%)被归类为失败。与失败风险增加相关的因素是术前矫正视力较差(OR = 2.46,P = 0.024)和术后眼压峰值(OR = 2.62,P = 0.028)。12只眼(9.5%)需要进一步手术来控制眼压。需要进一步手术控制眼压的危险因素是术前最高眼压(OR = 1.066,P = 0.047)和术后眼压峰值(OR = 4.531,P = 0.036)。GATT在各种青光眼类型中,无论是联合晶状体摘除还是作为独立手术,都在眼压和药物减少方面取得了良好的手术成功率。在药物治疗无法控制的青光眼治疗模式中,应尽早考虑GATT。