Chiariello Giovanni Alfonso, Di Mauro Michele, Villa Emmanuel, Bruno Piergiorgio, Mazza Andrea, Pavone Natalia, Nesta Marialisa, Marcolini Alberta, Panzera Rudy, Armonia Andrea, De Angelis Gaia, D'Avino Serena, Nenna Antonio, Pasquini Annalisa, Massetti Massimo
Department of Cardiovascular Sciences, Agostino Gemelli Foundation Polyclinic IRCCS, 00136 Rome, Italy.
Faculty of Medicine and Surgery, Catholic University of the Sacred Heart, 00168 Rome, Italy.
J Clin Med. 2025 May 15;14(10):3470. doi: 10.3390/jcm14103470.
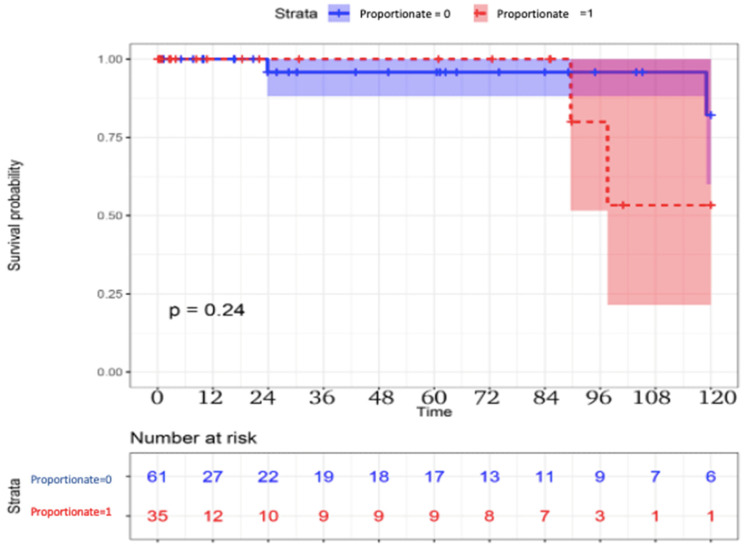
The treatment of secondary mitral regurgitation (MR) is still controversial. In 2019, a new conceptual framework was introduced, distinguishing between patients with a degree of MR "proportionate" to the left ventricular (LV) dilatation and patients in whom the severity of MR is "disproportionate" to the LV dilatation. The aim of this study was to compare the long-term outcome of patients with disproportionate vs. proportionate secondary MR who underwent mitral valve (MV) surgery. From January 2012 to June 2022, 96 patients with a preoperative diagnosis of pure secondary MR and LV dysfunction underwent MV surgery. The patients were divided in two groups, disproportionate vs. proportionate MR, according to echocardiographic parameters. A 5.2 (3.5-7.5) years complete clinical and echocardiographic follow-up was performed. In the study period, 61 patients with disproportionate and 35 patients with proportionate MR underwent surgical MV repair or MV replacement. The thirty-day outcome was comparable in the two groups. At long-term follow-up, mortality was 5% in the disproportionate group vs. 11% in the proportionate group ( = 0.2), and cardiovascular mortality was 3% vs. 9%, respectively (0.5). Rehospitalization for heart failure was 6% vs. 20% ( = 0.04), and the rate of patients with New York Heart Association (NYHA) functional class ≥ III was 8% vs. 26%, respectively ( = 0.01). LV volumes were significantly higher in the proportionate group, thus presenting a lower LV ejection fraction ( < 0.001 and = 0.03, respectively). No cases of recurrent MR have been observed. In this first exploratory analysis, patients with disproportionate secondary MR seem to present a possible benefit in terms of mortality and cardiovascular mortality, although not ones reaching statistical significance. Nevertheless, significant advantages were observed in terms of rehospitalization for heart failure, clinical status and symptoms, LV volumes, and LV function. Among patients referred to cardiac surgery, identifying the subset of patients with functional MR, who may obtain more significant advantages from surgery, seems relevant for patient selection, risk stratification, and to predict long-term outcomes.
继发性二尖瓣反流(MR)的治疗仍存在争议。2019年,引入了一个新的概念框架,区分二尖瓣反流程度与左心室(LV)扩张“相称”的患者和二尖瓣反流严重程度与左心室扩张“不相称”的患者。本研究的目的是比较接受二尖瓣(MV)手术的不相称与相称继发性MR患者的长期结局。2012年1月至2022年6月,96例术前诊断为单纯继发性MR和LV功能障碍的患者接受了MV手术。根据超声心动图参数,将患者分为不相称MR组和相称MR组。进行了5.2(3.5 - 7.5)年的完整临床和超声心动图随访。在研究期间,61例不相称MR患者和35例相称MR患者接受了手术MV修复或MV置换。两组的30天结局相当。在长期随访中,不相称组的死亡率为5%,相称组为11%(P = 0.2),心血管死亡率分别为3%和9%(P = 0.5)。因心力衰竭再次住院的比例分别为6%和20%(P = 0.04),纽约心脏协会(NYHA)功能分级≥III级的患者比例分别为8%和26%(P = 0.01)。相称组的LV容积显著更高,因此左心室射血分数更低(分别为P < 0.001和P = 0.03)。未观察到复发性MR病例。在这首次探索性分析中,不相称继发性MR患者在死亡率和心血管死亡率方面似乎有潜在益处,尽管未达到统计学意义。然而,在因心力衰竭再次住院、临床状态和症状、LV容积以及LV功能方面观察到了显著优势。在接受心脏手术的患者中,识别可能从手术中获得更显著益处的功能性MR患者亚组,对于患者选择、风险分层以及预测长期结局似乎具有重要意义。