Cimino Sara, Agati Luciano, Filomena Domenico, Maestrini Viviana, Monosilio Sara, Birtolo Lucia Ilaria, Mocci Michele, Mancone Massimo, Sardella Gennaro, Grayburn Paul, Fedele Francesco
Department of Clinical, Internal, Anesthesiological and Cardiovascular Sciences, Sapienza University of Rome, Policlinico Umberto I, 00161 Rome, Italy.
Division of Cardiology, Department of Internal Medicine, Baylor University Medical Center, Dallas, TX 75246, USA.
J Clin Med. 2022 Jan 27;11(3):645. doi: 10.3390/jcm11030645.
The impact of percutaneous mitral valve repair (PMVr) on long-term prognosis in patients with functional mitral regurgitation (FMR) is still unclear. Recently, a new conceptual framework classifying FMR as proportionate (P-MR) and disproportionate (D-MR) was proposed, according to the effective regurgitant orifice area/left ventricular end-diastolic volume (EROA/LVEDV) ratio. The aim was to assess its possible influence on PMVr efficacy.
A total of 56 patients were enrolled. MV annulus, LV volumes and function were assessed. Global longitudinal strain (GLS) was also calculated. Patients were divided into two groups, according to the EROA/LVEDV ratio. Echocardiographic follow-up was performed after 6 months, and adverse events were collected after 12 months.
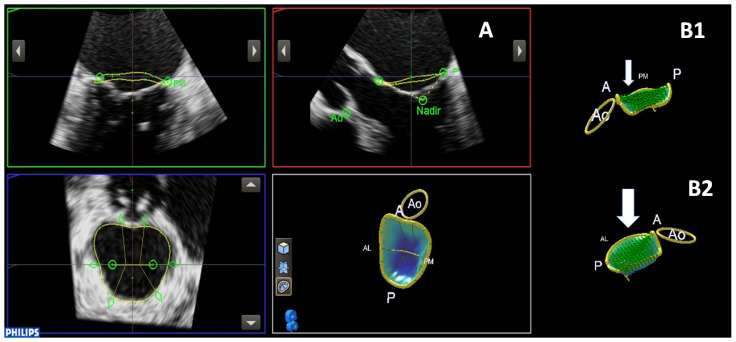
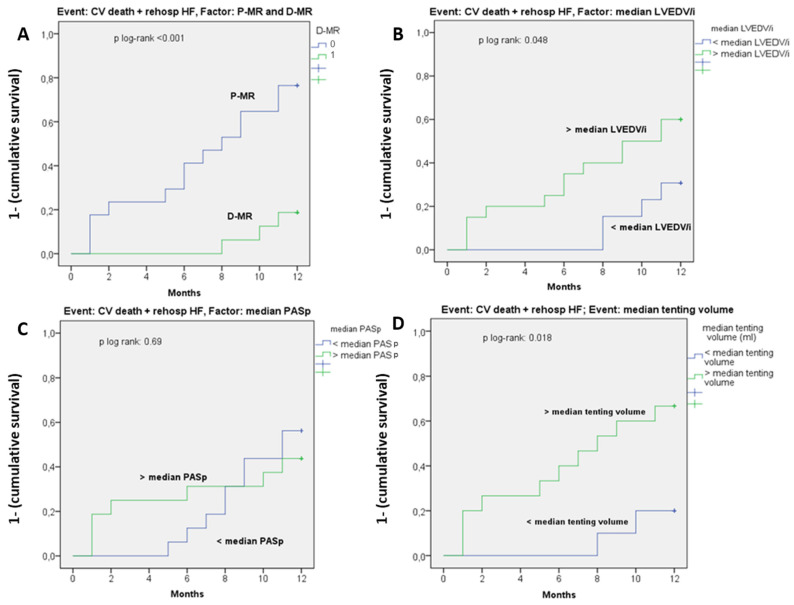
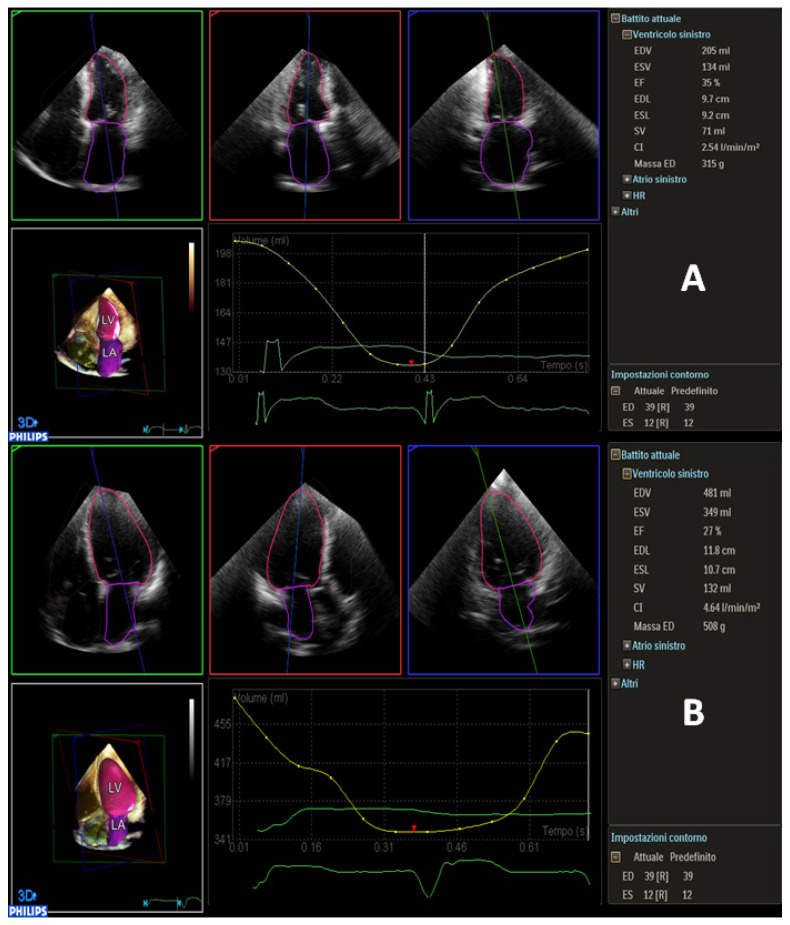
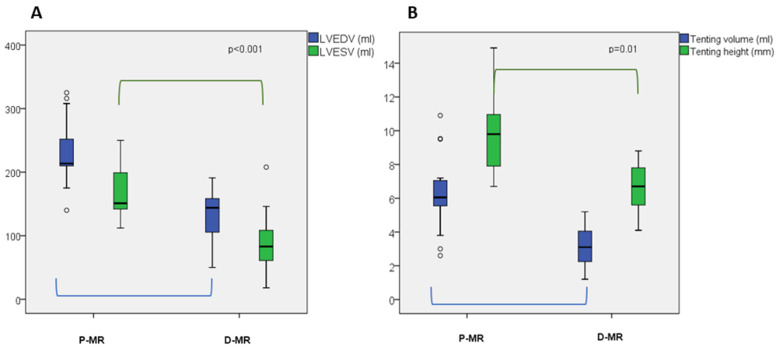
D-MR patients (n = 28, 50%) had a significantly more elliptical MV annulus ( = 0.048), lower tenting volume ( = 0.01), higher LV ejection fraction (LVEF: 32 ± 7 vs. 26 ± 5%, = 0.003), lower LVEDV, LV end-systolic volume (LVESV) and mass (LVEDV/i: 80 ± 20 vs. 126 ± 27 mL, = 0.001; LVESV/i: 60 ± 20 vs. 94 ± 23 mL, < 0.001; LV mass: 249 ± 63 vs. 301 ± 69 gr, = 0.035). GLS was more impaired in P-MR ( = 0.048). After 6 months, P-MR patients showed a higher rate of MR recurrence. After 12 months, the rate of CV death and rehospitalization due to HF was significantly higher in P-MR patients (46% vs. 7%, < 0.001). P-MR status was strongly associated with CV death/rehospitalization (HR = 3.4, CI 95% = 1.3-8.6, = 0.009).
Patients with P-MR seem to have worse outcomes after PVMr than D-MR patients. Our study confirms the importance of the EROA/LVEDV ratio in defining different subsets of FMR based on the anatomical characteristic of MV and LV.
经皮二尖瓣修复术(PMVr)对功能性二尖瓣反流(FMR)患者长期预后的影响仍不明确。最近,根据有效反流口面积/左心室舒张末期容积(EROA/LVEDV)比值,提出了一种将FMR分为比例性(P-MR)和非比例性(D-MR)的新概念框架。目的是评估其对PMVr疗效的可能影响。
共纳入56例患者。评估二尖瓣环、左心室容积和功能。还计算了整体纵向应变(GLS)。根据EROA/LVEDV比值将患者分为两组。6个月后进行超声心动图随访,12个月后收集不良事件。
D-MR患者(n = 28,50%)的二尖瓣环明显更呈椭圆形( = 0.048),帐篷样容积更低( = 0.01),左心室射血分数更高(LVEF:32±7 vs. 26±5%, = 0.003),左心室舒张末期容积、左心室收缩末期容积(LVESV)和质量更低(LVEDV/i:80±20 vs. 126±27 mL, = 0.001;LVESV/i:60±20 vs. 94±23 mL, < 0.001;左心室质量:249±63 vs. 301±69 gr, = 0.035)。P-MR患者的GLS受损更严重( = 0.048)。6个月后,P-MR患者的二尖瓣反流复发率更高。12个月后,P-MR患者因心力衰竭导致的心血管死亡和再住院率显著更高(46% vs. 7%, < 0.001)。P-MR状态与心血管死亡/再住院密切相关(HR = 3.4,95%CI = 1.3 - 8.6, = 0.009)。
P-MR患者在接受PVMr后的预后似乎比D-MR患者更差。我们的研究证实了EROA/LVEDV比值在根据二尖瓣和左心室的解剖特征定义FMR不同亚组中的重要性。