Canena Jorge, Pereira Pedro, Bana E Costa Tiago, Horta David, Lourenço Luís Carvalho, Rodrigues-Pinto Eduardo, Tarrio Isabel, Franco Ana Rita, Araújo Tarcísio, Lopes Luís
Hospital Cuf Tejo, University Center of Gastroenterology, Lisbon, Portugal.
Department of Gastroenterology, Hospital Prof. Doutor Fernando Fonseca, Amadora, Portugal.
GE Port J Gastroenterol. 2025 Apr 8:1-21. doi: 10.1159/000545718.
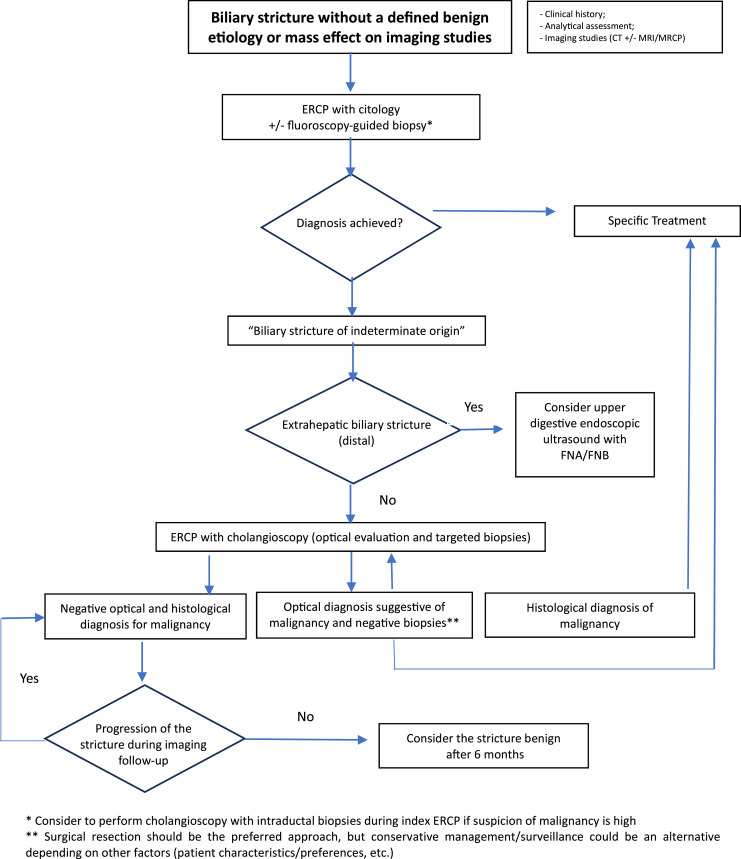
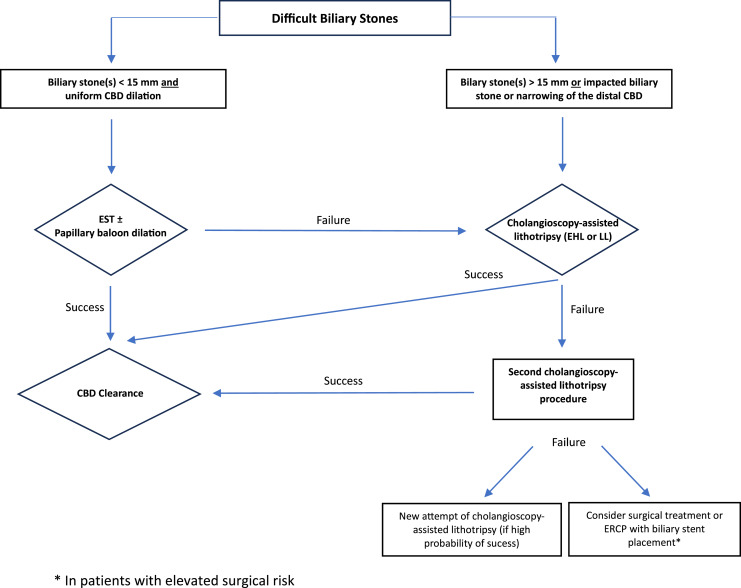
After a consensus meeting including experts from all over the country (more than 6 years of experience, at least 50 procedures and their center perform more than 30 procedures/year), several recommendations were issued. Main recommendations: (1) Single-operator digital cholangioscopy is indicated in cases of undetermined biliary strictures (UBSs) in which visual inspection, with or without histology, may change the patient's approach. (Strong recommendation, moderate quality of evidence). (2) In a cholangioscopy for a stricture of unclear etiology, the optical assessment aspects should be recorded in a standardized report and, according to the endoscopist's visual impression, suggest a malignant or benign etiology. (Strong recommendation, high quality of evidence). (3) When using cholangioscopy regardless of the visual impression, biopsies of the stenosis should be taken (ideally in a number equal to or greater than 6 fragments). (Strong recommendation, moderate quality of evidence). (4) Cholangioscopy with biopsies has a high diagnostic accuracy in the evaluation of UBSs, with a technical success >98% and visual diagnosis with sensitivity/specificity >95%. However, it must be considered that the sensitivity of histological diagnosis is lower (around 70%). (Strong recommendation, high quality of evidence). (5) The single-operator cholangioscopy (SOC)-assisted lithotripsy is a safe procedure associated with high rates of success. (Strong recommendation, high quality of evidence). (6) SOC-assisted lithotripsy should be reserved for selected cases in which conventional techniques for the treatment of difficult biliary stones have failed. However, SOC-assisted lithotripsy should be used early in the treatment algorithm to avoid repeated procedures. (Strong recommendation, moderate quality of evidence). (7) Pancreatoscopy can allow the diagnosis of lesions suggestive of malignancy in the pancreatic duct of patients with intraductal papillary mucinous neoplasm of the main duct with high sensitivity and specificity. The groups of patients who benefit most from its use are those with a diffusely dilated duct with a diameter greater than 10 mm, and in whom sectional imaging methods and endoscopic ultrasound do not reveal focal lesions. (Weak recommendation, low quality of evidence). (8) The use of intraductal lithotripsy guided by pancreatoscopy in patients with lithiasis in the main pancreatic duct should be reserved for patients with pain and lithiasis greater than 5 mm that cannot be removed using conventional techniques. Patients with an excessively distal location in the tail or head may cause increased technical difficulty. (Low recommendation, low quality of evidence).
在一次由来自全国各地的专家(拥有超过6年经验,至少完成50例手术且其所在中心每年完成超过30例手术)参加的共识会议之后,发布了若干建议。主要建议如下:(1)对于未明确的胆管狭窄(UBS)病例,若肉眼检查(无论有无组织学检查)可能改变患者的治疗方案,则建议采用单人操作数字胆管镜检查。(强烈推荐,证据质量中等)。(2)在针对病因不明的狭窄进行胆管镜检查时,光学评估方面应记录在标准化报告中,并根据内镜医师的肉眼印象,提示恶性或良性病因。(强烈推荐,证据质量高)。(3)无论肉眼印象如何,使用胆管镜检查时均应获取狭窄部位的活检样本(理想情况下数量等于或大于6块组织)。(强烈推荐,证据质量中等)。(4)胆管镜检查联合活检在评估UBS方面具有较高的诊断准确性,技术成功率>98%,肉眼诊断的敏感性/特异性>95%。然而,必须考虑到组织学诊断的敏感性较低(约70%)。(强烈推荐,证据质量高)。(5)单人操作胆管镜(SOC)辅助碎石术是一种安全的手术,成功率较高。(强烈推荐,证据质量高)。(6)SOC辅助碎石术应仅用于传统治疗复杂胆管结石技术失败的特定病例。然而,在治疗方案中应尽早使用SOC辅助碎石术以避免重复手术。(强烈推荐,证据质量中等)。(7)胰管镜检查可对主胰管内乳头状黏液性肿瘤患者的胰管内提示恶性的病变进行诊断,敏感性和特异性较高。从其使用中获益最大的患者群体是那些胰管弥漫性扩张且直径大于10mm,且断层成像方法和内镜超声未发现局灶性病变的患者。(弱推荐,证据质量低)。(8)对于主胰管结石患者,胰管镜引导下的胰管内碎石术应仅用于存在疼痛且结石大于5mm、无法用传统技术取出的患者。胰管结石位于胰尾或胰头过于远端的患者可能会增加技术难度。(低推荐,证据质量低)