Khateb Mohamed, Shelly Shahar
Department of Neurology, Rambam Medical Center, Haifa, Israel.
Department of Neurology, University Health Network (UHN), University of Toronto, Toronto, ON, Canada.
Front Neurol. 2025 May 14;16:1586031. doi: 10.3389/fneur.2025.1586031. eCollection 2025.
Although some reports link Myasthenia Gravis to higher mortality, the evidence remains contradictory and unclear. Real-life data is limited primarily due to challenges in selecting control groups and mitigating bias. Additionally, a revised mortality assessment should be conducted due to recent advancements in Myasthenia Gravis treatments over the past decade, including new biological therapies and the impact of the COVID-19 pandemic from 2020 to 2023.
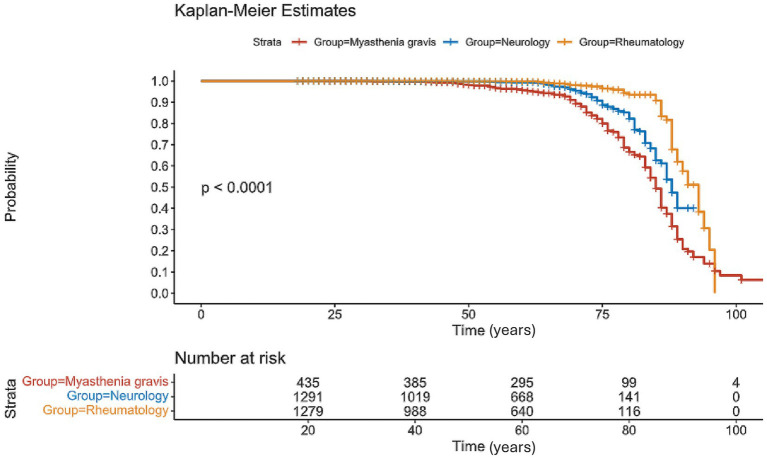
We conducted a retrospective analysis of all patients diagnosed with Myasthenia Gravis at our tertiary center between 2000 and 2023, extracting mortality and clinical features compared to two age- and sex-matched control groups of neurological or rheumatologic patients.
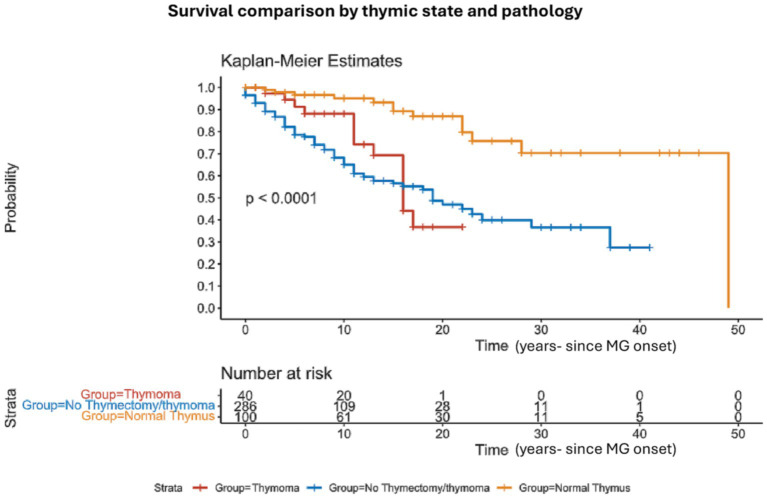
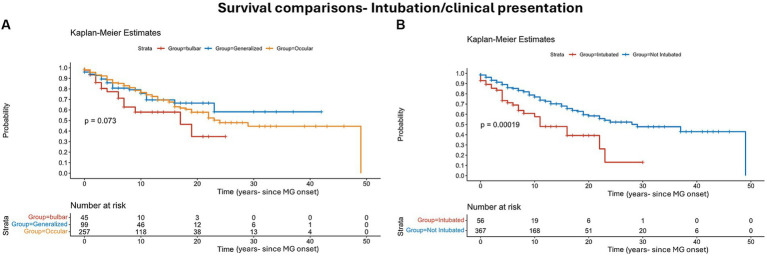
We identified 436 Myasthenic patients and 2,616 controls (1308 in each control group). Myasthenia Gravis mortality was 14% at 5 years (61/422) and 21% at 10 years (87/422). Mortality was significantly higher than control groups ( < 0.001). Intubations during myasthenic crisis were linked to higher mortality ( = 0.002). Bulbar weakness at presentation showed higher mortality but did not reach clinical significance. We compared the mean age at death in MG patients to national life expectancy benchmarks using a one-sample Z-test, revealing significantly younger age at death in both males (78.3 vs. 81.6 years, = 0.009) and females (76.5 vs. 85.2 years, < 0.00001). Patients with normal thymic pathology showed better outcomes and lower mortality after thymic removal ( < 0.0001). The primary cause of death was linked to infections, significantly correlated with chronic steroid use.
In conclusion, patients with Myasthenia Gravis had higher mortality rates. Thymic removal reduced mortality, while intubation is associated with increased mortality risk.
尽管一些报告将重症肌无力与更高的死亡率联系起来,但证据仍然相互矛盾且不明确。现实生活中的数据有限,主要是由于在选择对照组和减轻偏差方面存在挑战。此外,由于过去十年重症肌无力治疗的最新进展,包括新的生物疗法以及2020年至2023年新冠疫情的影响,应进行修订后的死亡率评估。
我们对2000年至2023年期间在我们的三级中心诊断为重症肌无力的所有患者进行了回顾性分析,提取了死亡率和临床特征,并与两个年龄和性别匹配的神经科或风湿科患者对照组进行比较。
我们确定了436例重症肌无力患者和2616例对照组(每个对照组1308例)。重症肌无力患者5年死亡率为14%(61/422),10年死亡率为21%(87/422)。死亡率显著高于对照组(<0.001)。重症肌无力危象期间的插管与更高的死亡率相关(=0.002)。就诊时的延髓肌无力显示出更高的死亡率,但未达到临床显著性。我们使用单样本Z检验将重症肌无力患者的平均死亡年龄与国家预期寿命基准进行比较,结果显示男性(78.3岁对81.6岁,=0.009)和女性(76.5岁对85.2岁,<0.00001)的死亡年龄均显著更年轻。胸腺病理正常的患者在胸腺切除术后预后更好,死亡率更低(<0.0001)。主要死亡原因与感染有关,与长期使用类固醇显著相关。
总之,重症肌无力患者的死亡率较高。胸腺切除可降低死亡率,而插管与死亡风险增加有关。