Palhares Guilherme M, Retzky Julia S, Coxe Francesca, Hinkley Paige, Rizy Morgan E, Neijna Ava G, Gomoll Andreas H, Strickland Sabrina M
Sports Medicine Institute, Hospital for Special Surgery, New York, New York, USA.
Orthop J Sports Med. 2025 May 29;13(5):23259671251341474. doi: 10.1177/23259671251341474. eCollection 2025 May.
Third-generation autologous chondrocyte implantation (ACI), also known as matrix-induced ACI (MACI), was approved for clinical practice in December 2016. Studies specifically investigating outcomes of MACI for complex patellofemoral chondral lesions are limited.
To report patient-reported outcome measures (PROMs), complications, and failure rates after MACI for patellofemoral chondral defects at a minimum follow-up of 2 years.
Case series; Level of evidence, 4.
For this retrospective review of prospectively collected data, the authors identified patients who underwent treatment with MACI for focal chondral defects in the knee between August 2017 and September 2020. PROMs, including International Knee Documentation Committee (IKDC) score, Kujala score for patellofemoral disorders, and the Veterans RAND 12-item Health Survey (VR-12) score, were obtained preoperatively and a minimum of 2 years postoperatively. The percentage of patients who met the minimal clinically important difference (MCID) for each PROM was reported. Failure was defined as (1) graft failure on follow-up magnetic resonance imaging or second-look arthroscopy, (2) revision MACI or other chondral procedure, or (3) conversion to unicompartmental or total knee arthroplasty.
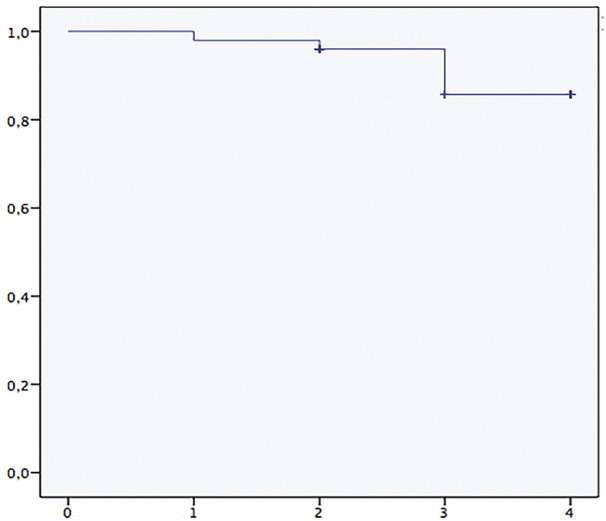
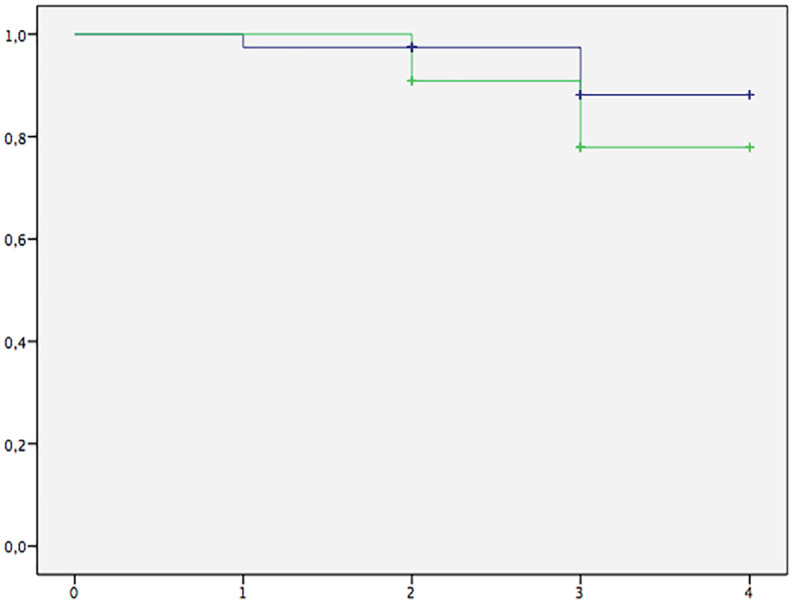
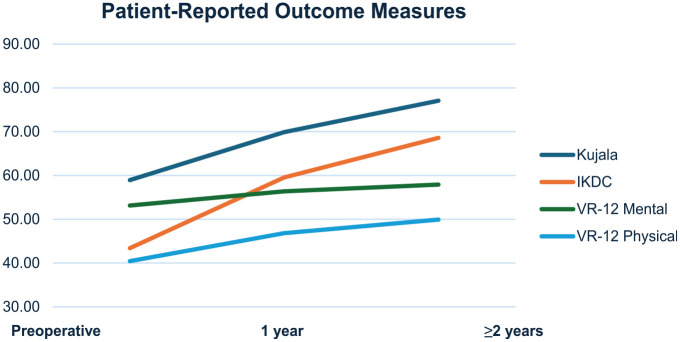
A total of 50 patients (34 female; mean age, 32.43 ± 7.33 years; mean follow-up, 2.71 ± 0.79 years) remained after application of the exclusion criteria. There was a significant increase in all PROMs from preoperatively to postoperatively, including the IKDC (43.39 vs 68.58; < .001), Kujala (58.93 vs 77.07; < .001), VR-12 Mental (53.12 vs 57.90; = .002), and VR-12 Physical (40.40 vs 49.89; < .001) scores, with 5 (10%) failures. The MCID was achieved by 77.8% of patients in IKDC score and 69.0% in the Kujala score. Kaplan-Meier survival analysis showed survival probabilities of 98.0%, 96.0%, and 85.7% at 1, 2, and 4 years, respectively. MACI for patellofemoral bipolar lesions (n = 11) showed significant improvement in IKDC (50.06 vs 74.07; = .008) and Kujala (69.33 vs 84.33; = .046) scores, and 2 (18.2%) failures. Kaplan-Meier survival analysis with log-rank test demonstrated no significant differences in survival distributions between unipolar and bipolar patellofemoral lesions ( = .387).
Third-generation ACI (MACI) is a successful and effective treatment method for difficult-to-treat patellar, trochlear, and bipolar patellofemoral chondral defects.
第三代自体软骨细胞移植术(ACI),也称为基质诱导ACI(MACI),于2016年12月被批准用于临床实践。专门研究MACI治疗复杂髌股关节软骨损伤疗效的研究有限。
报告MACI治疗髌股关节软骨缺损至少2年随访后的患者报告结局指标(PROMs)、并发症及失败率。
病例系列研究;证据等级,4级。
在对前瞻性收集的数据进行的这项回顾性研究中,作者确定了2017年8月至2020年9月期间接受MACI治疗膝关节局灶性软骨缺损的患者。术前及术后至少2年获取PROMs,包括国际膝关节文献委员会(IKDC)评分、髌股关节疾病的库贾拉评分以及退伍军人兰德12项健康调查(VR-12)评分。报告达到每个PROM最小临床重要差异(MCID)的患者百分比。失败定义为:(1)随访磁共振成像或二次关节镜检查时移植物失败;(2)翻修MACI或其他软骨手术;(3)转换为单髁或全膝关节置换术。
应用排除标准后,共有50例患者(34例女性;平均年龄32.43±7.33岁;平均随访2.71±0.79年)。从术前到术后,所有PROMs均有显著提高,包括IKDC评分(43.39对68.58;P<.001)、库贾拉评分(58.93对77.07;P<.001)、VR-12精神健康评分(53.12对57.90;P = .002)和VR-12身体健康评分(40.40对49.89;P<.001),有5例(10%)失败。IKDC评分中77.8%的患者及库贾拉评分中69.0%的患者达到了MCID。Kaplan-Meier生存分析显示,1年、2年和4年的生存概率分别为98.0%、96.0%和85.7%。髌股关节双极损伤患者(n = 11)接受MACI治疗后,IKDC评分(50.06对74.07;P = .008)和库贾拉评分(69.33对84.33;P = .046)有显著改善,2例(18.2%)失败。采用对数秩检验的Kaplan-Meier生存分析表明,单极和双极髌股关节损伤的生存分布无显著差异(P = .387)。
第三代ACI(MACI)是治疗难治性髌骨、滑车及双极髌股关节软骨缺损的一种成功且有效的治疗方法。