Ferrada Paula, Shafique Saima, Brenner Megan, Burlew Clay, Catena Fausto, Coleman Julia, Coleman Jamie, Demetriades Demetrios, Demoya Marc, Di Saverio Salomone, Dissanaike Sharmila, Dransfield Tom, DuBose Joseph, Duchesne Juan, Elkbuli Adel, Foianini Esteban, Gambardella Josephine, Garcia Alberto, Goldberg Amy, Goralnick Eric, Holcomb John, Jonathan Messing, Joseph Bellal, Jacobs Lenworth, Kerby Jeffrey, Lawerance Robert, Leichtle Stefan, Lucas Charles, Machain Gustavo, Macleod Jana, Maher Zoe, Martin Matthew, Mendez Napoleon, Menegozzo Carlos, Merlini Ilenia, Namias Nicholas, Narayan Mayur, Ordonez Carlos, Ottolino Pablo, Patel Mayur, Qasim Zaffer A, Quiodettis Martha, Young LeAnne Sitari, Ratnasekera Ashanti, Rayburn David, Salamea Juan, Sarani Babak, Scalea Thomas, Seamon Mark, Spain David, Steele Portia, Taghavi Sharven, Tatebe Leah, Vega Felipe, Velmahos George, Zakrison Tanya, Biffl Walter L, Damaskos Dimitrios, Coccolini Federico, Vallicelli Carlo, Moore Ernest E, Ansaloni Luca, Kluger Yoram
Inova Healthcare System, 3300 Gallows Road, Falls Church, VA, USA.
University of Virginia, Charlottesville, USA.
World J Emerg Surg. 2025 Jun 2;20(1):47. doi: 10.1186/s13017-025-00618-2.
Hemorrhage is one of the leading causes of preventable death in trauma patients. For decades, the Airway-Breathing-Circulation (ABC) approach has been the cornerstone of trauma care. However, emerging evidence suggests that prioritizing airway management in exsanguinating patients may worsen hypotension and increase mortality. This systematic review and meta-analysis aim to evaluate the effectiveness of the Circulation-Airway-Breathing (CAB) approach compared to the traditional ABC sequence in improving survival in trauma patients with severe hemorrhage.
A systematic review was conducted in accordance with the PRISMA guidelines. Databases including PubMed and Ovid MEDLINE, SCOPUS, web of science and EMBASE were searched for studies published up to September 2024. Eligible studies included observational and comparative studies reporting outcomes of trauma patients with exsanguinating hemorrhage. The Newcastle-Ottawa Scale was used for risk of bias assessment. A meta-analysis was performed using a random-effects model to calculate pooled odds ratios (OR) for mortality, with 95% confidence intervals (CI). Subgroup analysis was conducted to compare the ABC and CAB approaches in prospective and retrospective studies.
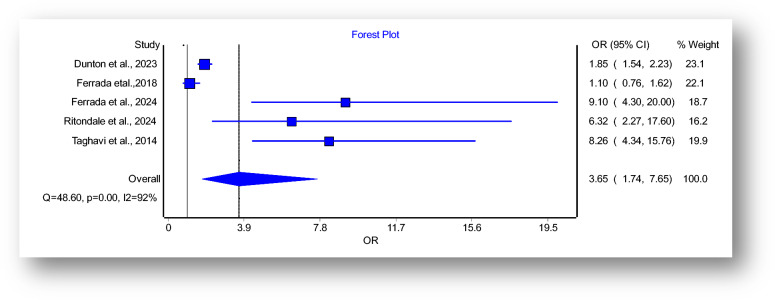
Six studies (N = 11,855 patients) met the inclusion criteria. The meta-analysis revealed a significant increase in mortality associated with the ABC approach (pooled OR: 3.65, 95% CI: 1.74-7.65). Subgroup analysis of prospective cohort studies found an even higher mortality risk (POR: 9.99, 95% CI: 5.59-17.85) when compared with POR of retrospective studies (POR: 2.42, 95%CI: 1.08-5.36). High heterogeneity (I2 = 92%) was observed across the studies, likely due to variations in patient populations and resuscitation protocols.
Prioritizing circulation over airway management in trauma patients with exsanguinating injuries significantly reduces mortality compared to the traditional ABC approach. The present consensus paper, conducted according to the WSES methodology, aims to provide a review of the literature comparing the CAB approach to the traditional ABC sequence in trauma patients with exsanguinating hemorrhage, to develop a shared consensus statement based on the currently available evidence.
出血是创伤患者可预防死亡的主要原因之一。几十年来,气道-呼吸-循环(ABC)方法一直是创伤护理的基石。然而,越来越多的证据表明,在大出血患者中优先进行气道管理可能会加重低血压并增加死亡率。本系统评价和荟萃分析旨在评估与传统ABC顺序相比,循环-气道-呼吸(CAB)方法在提高严重出血创伤患者生存率方面的有效性。
按照PRISMA指南进行系统评价。检索了包括PubMed、Ovid MEDLINE、SCOPUS、科学网和EMBASE在内的数据库,以查找截至2024年9月发表的研究。符合条件的研究包括报告大出血创伤患者结局的观察性和比较性研究。使用纽卡斯尔-渥太华量表进行偏倚风险评估。采用随机效应模型进行荟萃分析,以计算死亡率的合并比值比(OR)及95%置信区间(CI)。进行亚组分析,以比较前瞻性和回顾性研究中的ABC和CAB方法。
六项研究(N = 11855例患者)符合纳入标准。荟萃分析显示,ABC方法与死亡率显著增加相关(合并OR:3.65,95% CI:1.74 - 7.65)。前瞻性队列研究的亚组分析发现,与回顾性研究的比值比(POR:2.42,95% CI:1.08 - 5.36)相比,死亡风险更高(POR:9.99,95% CI:5.59 - 17.85)。各研究间观察到高度异质性(I2 = 92%),可能是由于患者群体和复苏方案的差异所致。
与传统ABC方法相比,在大出血创伤患者中优先进行循环管理而非气道管理可显著降低死亡率。本共识文件根据WSES方法编写,旨在综述比较CAB方法与传统ABC顺序在大出血创伤患者中的文献,以便根据现有证据制定共同的共识声明。