Shi Jinchuan, Zhang Wenhui, Han Jie, Zhang Zhongdong, Yan Dingyan, Zheng Rongrong, Li Feng, Wang Yi
Department of Infection, Affiliated Hangzhou Xixi Hospital, Zhejiang Chinese Medical University, Hangzhou, 310023, People's Republic of China.
Department of Nursing, Affiliated Hangzhou Xixi Hospital, Zhejiang Chinese Medical University, Hangzhou, 310023, People's Republic of China.
Infect Drug Resist. 2025 May 29;18:2703-2716. doi: 10.2147/IDR.S516775. eCollection 2025.
Both B/F/TAF and DTG/3TC are recommended in treatment guidelines for switch therapy in PLWH. This study aimed to evaluate the safety and metabolic health consequences of two switched regimens in a real-world setting among virologically suppressed PLWH previously treated with EFV/TDF/3TC.
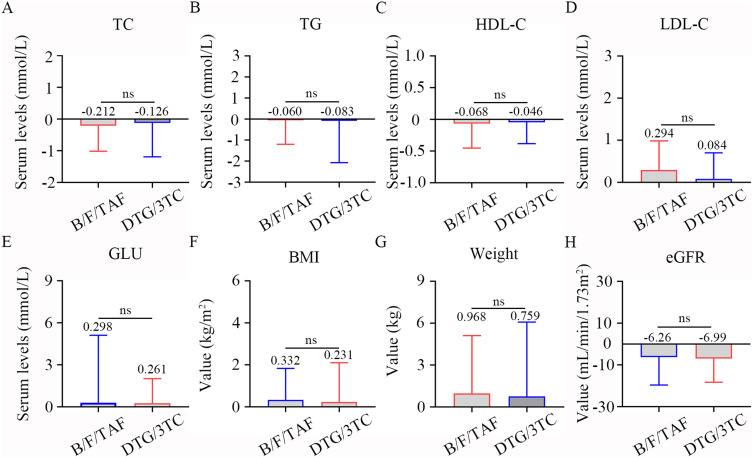
This retrospective real-world study in Hangzhou included 220 virologically suppressed PLWH who switched from EFV/TDF/3TC to DTG/3TC or B/F/TAF between January 1, 2020 and October 30, 2023. All participants were examined the changes in weight, BMI, GLU levels, lipid parameters (TC, LDL-C, HDL-C, and TG), and eGFR at post-12-month.
The mean age of included participants was 50.8 years (SD: 11.3). After 12 months of switching, the HIV RNA level was below the limit of detection (< 20 copies/mL) among all participants. The switch to DTG/3TC or B/F/TAF therapy was associated with significant improvement in LDL-C, GLU levels, and eGFR values (all < 0.05), while other metabolic indexes did not change significantly. Furthermore, there was a significant difference in the incidence of hyperglycemia (5.7% vs 19.35%; = 0.004) between the B/F/TAF and DTG/3TC groups, but not included the mean changes of weight, BMI, lipid profiles, GLU levels, and eGFR and incidence of high TC and high TG. For the aged 40-59 years and aged ≥ 60 years PLWH, the differences in metabolic indicators were minimal between DTG/3TC and B/F/TAF groups post-12-month, with no significant differences between the arms in mean change from baseline in TC, TG, HDL-C, LDL-C, GLU, BMI, weight, and eGFR.
In this study, the B/F/TAF or DTG/3TC regimens are safe for virologically suppressed PLWH aged > 40 years. The transition to B/F/TAF demonstrated dual clinical benefits, significantly reducing hyperglycemia incidence while preserving renal function.
B/F/TAF和DTG/3TC均被推荐用于HIV感染者(PLWH)转换治疗的指南中。本研究旨在评估在真实世界环境中,两种转换方案对先前接受EFV/TDF/3TC治疗且病毒学抑制的PLWH的安全性和代谢健康影响。
这项在杭州开展的回顾性真实世界研究纳入了220例病毒学抑制的PLWH,他们在2020年1月1日至2023年10月30日期间从EFV/TDF/3TC转换为DTG/3TC或B/F/TAF。所有参与者在转换12个月后接受体重、BMI、血糖水平、血脂参数(总胆固醇、低密度脂蛋白胆固醇、高密度脂蛋白胆固醇和甘油三酯)以及估算肾小球滤过率(eGFR)变化的检查。
纳入参与者的平均年龄为50.8岁(标准差:11.3)。转换治疗12个月后,所有参与者的HIV RNA水平均低于检测下限(<20拷贝/mL)。转换为DTG/3TC或B/F/TAF治疗与低密度脂蛋白胆固醇、血糖水平和eGFR值显著改善相关(均P<0.05),而其他代谢指标无显著变化。此外,B/F/TAF组和DTG/3TC组之间高血糖发生率存在显著差异(5.7%对19.35%;P=0.004),但体重、BMI、血脂谱、血糖水平、eGFR的平均变化以及高总胆固醇和高甘油三酯的发生率无差异。对于年龄在40 - 59岁和≥60岁的PLWH,转换12个月后DTG/3TC组和B/F/TAF组之间的代谢指标差异最小,两组之间总胆固醇、甘油三酯、高密度脂蛋白胆固醇、低密度脂蛋白胆固醇、血糖、BMI、体重和eGFR从基线的平均变化无显著差异。
在本研究中,B/F/TAF或DTG/3TC方案对年龄>40岁且病毒学抑制的PLWH是安全的。转换为B/F/TAF显示出双重临床益处,显著降低高血糖发生率同时保留肾功能。