Parnasa Shani Y, Shweiki Amir, Pinhasov Diana, Abu Salem Samer, Gefen Rachel, Mizrahi Ido, Abu-Gazala Mahmoud, Pikarsky Alon J, Shussman Noam
Department of General Surgery, Hadassah Medical Organization and Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel.
Int J Colorectal Dis. 2025 Jun 3;40(1):134. doi: 10.1007/s00384-025-04926-6.
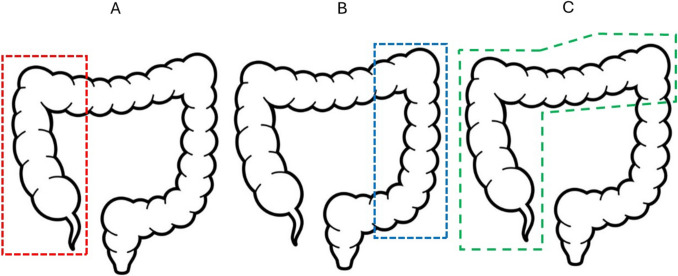
Prolonged postoperative ileus (PPOI) is associated with a lengthy hospital stay, risk of additional complications and substantial costs. Data regarding the incidence of PPOI following right extended colectomy (REC) with ileo-descending anastomosis is limited. This study aimed to compare the incidence of PPOI and evaluate risk factors for this condition among patients undergoing REC, left hemicolectomy (LC), and right hemicolectomy (RC) for colon carcinoma.
This retrospective, single-center cohort study included patients who underwent colectomy for cancer at our institution between January 2014 and January 2022. Outcome measures were postoperative time to first bowel movement and flatus, postoperative time to tolerate a solid low-residue diet, the need for nasogastric tube (NGT) decompression or total parenteral nutrition (TPN), and length of hospital stay (LOS).
A total of 534 patients were included: 242 (45.3%) underwent LC, 207 (38.8%) RC, and 85 (15.9%) REC. There were no significant differences in surgical approach (laparoscopic vs. open), operative time, percentage of urgent surgeries, postoperative complication rates, or advanced T stages among the groups. Compared with LC and RC, REC was associated with a longer time to first flatus (p = 0.04), delayed tolerance of a solid diet (p < 0.001), and increased LOS (p < 0.001). Patients following REC were at a higher risk for the need of NGT decompression (p = 0.003). Analysis of covariance controlling for potential confounding variables identified REC as an independent risk factor for PPOI following surgery.
This study revealed a higher incidence of PPOI following REC for cancer compared to RC and LC.
术后肠梗阻持续时间延长(PPOI)与住院时间延长、额外并发症风险及高额费用相关。关于回肠降结肠吻合术的右半结肠扩大切除术(REC)后PPOI发生率的数据有限。本研究旨在比较接受REC、左半结肠切除术(LC)和右半结肠切除术(RC)治疗结肠癌患者的PPOI发生率,并评估该疾病的危险因素。
这项回顾性单中心队列研究纳入了2014年1月至2022年1月期间在本机构接受结肠癌结肠切除术的患者。观察指标包括术后首次排便和排气时间、术后耐受低渣固体饮食的时间、是否需要鼻胃管(NGT)减压或全胃肠外营养(TPN)以及住院时间(LOS)。
共纳入534例患者:242例(45.3%)接受LC,207例(38.8%)接受RC,85例(15.9%)接受REC。各组之间在手术方式(腹腔镜与开放手术)、手术时间、急诊手术百分比、术后并发症发生率或T分期较晚方面无显著差异。与LC和RC相比,REC与首次排气时间延长(p = 0.04)、固体饮食耐受延迟(p < 0.001)及住院时间延长(p < 0.001)相关。REC患者需要NGT减压的风险更高(p = 0.003)。对潜在混杂变量进行协方差分析后确定REC是术后PPOI的独立危险因素。
本研究显示,与RC和LC相比,REC治疗癌症后PPOI的发生率更高。