Polito Maria Vincenza, Esposito Alessandra Maria, Barbato Maria Grazia, Ferrara Francesco
Division of Cardiology, "Cava de' Tirreni and Amalfi Coast" Hospital, Heart Department, University Hospital of Salerno, Baronissi, SA, Italy.
Department of Medicine, Surgery and Dentistry, University of Salerno, Baronissi, SA, Italy.
J Cardiovasc Echogr. 2025 Jan-Mar;35(1):69-73. doi: 10.4103/jcecho.jcecho_69_24. Epub 2025 Apr 30.
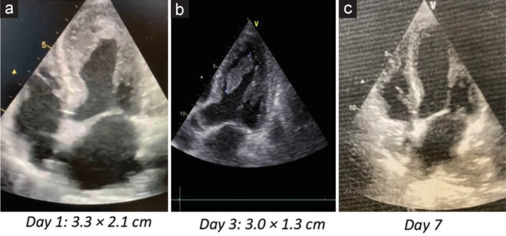
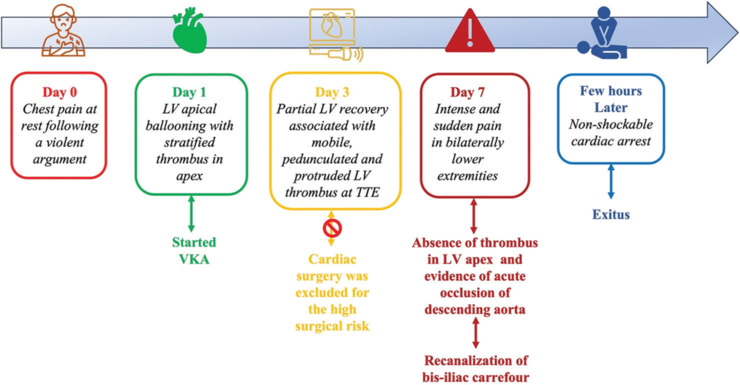
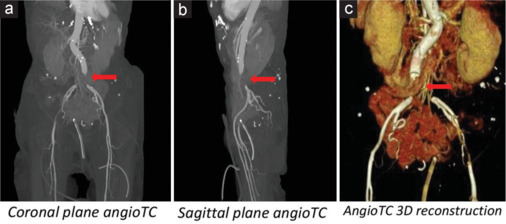
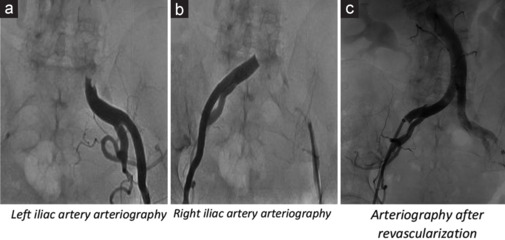
Left ventricular thrombosis (LVT) in stress cardiomyopathy or Takotsubo syndrome (TTS) is a moderately frequent complication. However, cardioembolic events are not frequently reported. Herein, we present a case report of 80-year-old patient admitted for chest pain at rest, started few days earlier following a violent argument. Her medical history included arterial hypertension and recent surgery of descending colon adenocarcinoma. Electrocardiogram showed sinus rhythm, negative T waves from V1 to V6, in D2, D3, AVF, and long QTc. Laboratory examinations documented an increased high sensitivity Troponin I, myoglobin, creatine kinase-MB, and B-type natriuretic peptide. Transthoracic echocardiography (TTE) showed a reduced left ventricular (LV) ejection fraction, "apical ballooning" with hyperkinesis of the basal segments of LV, suggestive for stress cardiomyopathy. A large thrombus in LV apex (3.3 cm × 2.1 cm) was found. Coronary angiogram showed normal coronary arteries. Anticoagulant therapy with Warfarin was quickly started, bridging with unfractionated heparin. Cardiac surgery was excluded for high-risk surgical patient. Daily TTE monitoring was done with evidence of slight reduction of the LVT. After 7 day from admission, the patient complained an intense and sudden pain in lower extremities bilaterally. An acute occlusion of the descending aorta just above the bifurcation in the common iliac arteries was found. Interventional radiology procedure of recanalization of the bis-iliac carrefour was successfully performed. However, few hours after the procedure, the patient's hemodynamic conditions worsened until the exitus.
应激性心肌病或Takotsubo综合征(TTS)中的左心室血栓形成(LVT)是一种较为常见的并发症。然而,心脏栓塞事件的报道并不常见。在此,我们报告一例80岁患者,因静息时胸痛入院,胸痛始于几天前的一次激烈争吵之后。她的病史包括动脉高血压和近期降结肠癌手术。心电图显示窦性心律,V1至V6、D2、D3、AVF导联T波倒置,QTc间期延长。实验室检查显示高敏肌钙蛋白I、肌红蛋白、肌酸激酶-MB和B型利钠肽升高。经胸超声心动图(TTE)显示左心室(LV)射血分数降低,LV基底部节段运动亢进伴“心尖部气球样变”,提示应激性心肌病。在LV心尖部发现一个大血栓(3.3 cm×2.1 cm)。冠状动脉造影显示冠状动脉正常。迅速开始使用华法林进行抗凝治疗,并使用普通肝素进行桥接。因患者手术风险高,排除心脏手术。每天进行TTE监测,结果显示LVT略有缩小。入院7天后,患者双侧下肢突然剧烈疼痛。发现腹主动脉在双侧髂总动脉分叉上方急性闭塞。成功进行了双侧髂动脉分叉处再通的介入放射学手术。然而,手术后数小时,患者的血流动力学状况恶化直至死亡。