Dontsova Valeriya, Mohan Haneesha, Yee Audrey, Nguyen Jessica, Fahmida Maisha, Greene Nicholas D E, Copp Andrew J, Zash Rebecca, Jao Jennifer, Serghides Lena
Toronto General Hospital Research Institute, Princess Margaret Cancer Research Tower (PMCRT), University Health Network, 101 College Street, 10th Floor, Room, 359, Toronto, ON, M5G 1L7, Canada.
Developmental Biology and Cancer Department, UCL Great Ormond Street Institute of Child Health, University College London, London, UK.
Sci Rep. 2025 Jun 4;15(1):19601. doi: 10.1038/s41598-025-02130-8.
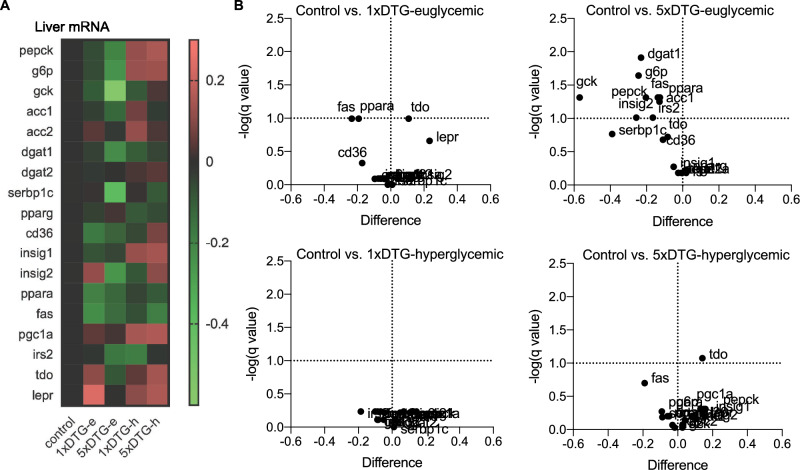
Dolutegravir (DTG), is recommended for all people with HIV, including pregnant women. Weight gain and hyperglycemia have been reported with DTG use, as well as a signal for neural tube defects (NTDs) that has waned over time. Obesity and hyperglycemia are risk factors for NTDs. We explored the impact of DTG-based antiretroviral therapy (ART) on weight gain and glucose homeostasis in female mice. C57BL/6 mice were treated daily for 9 weeks with water (control), 1xDTG (2.5 mg/kg DTG + 33.3/50 mg/kg emtricitabine/tenofovir-yielding therapeutic levels), or 5xDTG (12.5 mg/kg + 33.3/50 mg/kg emtricitabine/tenofovir). Overnight fasted glucose, weight, and oral glucose tolerance test (OGTT) were measured at 2-8 weeks. Tissue was collected for expression analyses of glucose homeostasis pathways. Weight gain was similar between groups. We observed a transient fasted hyperglycemia with DTG treatment, that peaked at week 6 and resolved by week 9. No significant differences were observed in insulin or OGTT response between groups. DTG was associated with a gradual and persistent decrease in plasma leptin and increase in plasma corticosterone levels compared to controls. Downregulation of genes involved in gluconeogenesis and lipogenesis in liver were observed in DTG-treated mice that remained euglycemic. Muscle and liver leptin receptor expression was elevated with DTG treatment. DTG was associated with transient hyperglycemia, lower leptin and higher corticosterone. Induction of compensatory mechanisms may have aided to restore/maintain euglycemia. This transient nature of the glycemic dysregulation may in part explain the loss of the NTD signal that was observed at the initial roll out of DTG but waned over time.
多替拉韦(DTG)被推荐用于所有艾滋病毒感染者,包括孕妇。有报道称使用DTG会出现体重增加和高血糖,以及随着时间推移已减弱的神经管缺陷(NTD)信号。肥胖和高血糖是NTD的危险因素。我们探讨了基于DTG的抗逆转录病毒疗法(ART)对雌性小鼠体重增加和葡萄糖稳态的影响。将C57BL/6小鼠每天用水(对照)、1倍剂量DTG(2.5毫克/千克DTG + 33.3/50毫克/千克恩曲他滨/替诺福韦,产生治疗水平)或5倍剂量DTG(12.5毫克/千克 + 33.3/50毫克/千克恩曲他滨/替诺福韦)处理9周。在第2至8周测量过夜禁食血糖、体重和口服葡萄糖耐量试验(OGTT)。收集组织用于葡萄糖稳态途径的表达分析。各组之间体重增加相似。我们观察到DTG治疗会出现短暂的空腹高血糖,在第6周达到峰值并在第9周恢复。各组之间在胰岛素或OGTT反应方面未观察到显著差异。与对照组相比,DTG与血浆瘦素逐渐持续下降和血浆皮质酮水平升高有关。在血糖正常的DTG处理小鼠中观察到肝脏中参与糖异生和脂肪生成的基因下调。DTG处理使肌肉和肝脏瘦素受体表达升高。DTG与短暂性高血糖、较低的瘦素和较高的皮质酮有关。代偿机制的诱导可能有助于恢复/维持血糖正常。这种血糖失调的短暂性质可能部分解释了在DTG最初推出时观察到的NTD信号的消失,但随着时间推移该信号减弱。