Briscoe Simon, Shaw Elizabeth, Nunns Michael, Lawal Hassanat, Orr Noreen, Coon Jo Thompson, Garside Ruth, Melendez-Torres G J
Exeter PRP Evidence Review Facility, University of Exeter Medical School University of Exeter Exeter UK.
Cochrane Evid Synth Methods. 2024 Apr 3;2(4):e12052. doi: 10.1002/cesm.12052. eCollection 2024 Apr.
Health inequities are systematic, avoidable, and unfair differences in health between populations or population subgroups. There is increased recognition of the need for systematic reviews (SRs) to address health inequities, including drawing out findings relevant to low- and middle-income countries (LMICs). The aim of this study was to determine the extent to which SRs on risk factors for hearing loss reported findings associated with health inequities, and the extent to which this data was captured in the primary studies included within these SRs.
We identified SRs on risk factors for hearing loss from a report on this topic which included a systematic search for relevant SRs. SRs thus identified were inspected for data related to health inequity with reference to PROGRESS-Plus. We compared how data were reported in SRs versus within primary studies included in the SRs, and the extent to which primary studies from LMICs were represented.
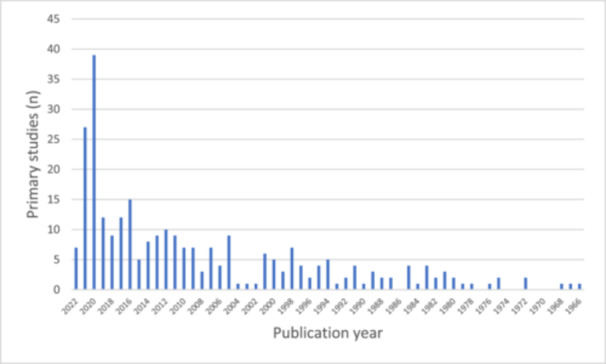
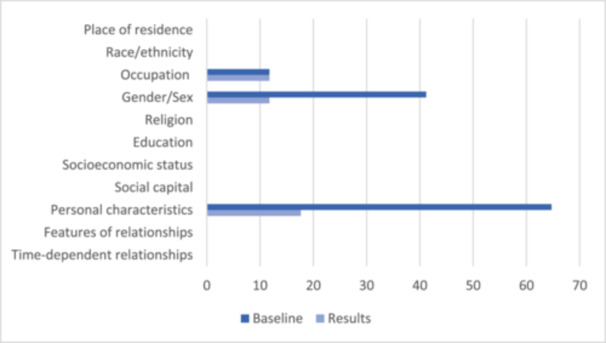
We included 17 SRs which reported findings on a variety of physiological, behavioral, demographic, and environmental risk factors for hearing loss. There were 296 unique primary studies included in the SRs, of which 251 (81.49%) were successfully retrieved. Data relating to health inequities was reported relatively infrequently in the SRs and mainly focused on gender and age. Data related to health inequities was more frequently reported in primary studies. However, several PROGRESS-Plus criteria were only reported in a minority of primary studies. Approximately one-third of primary studies were from LMICs.
There is scope to improve the reporting of data relating to health inequities in primary studies on risk factors for hearing loss. However, SR authors could do more to report health inequities than is currently undertaken, including drawing out findings relevant to LMICs where data are available.
健康不平等是不同人群或人群亚组之间在健康方面存在的系统性、可避免且不公平的差异。人们越来越认识到需要进行系统评价(SRs)来解决健康不平等问题,包括梳理出与低收入和中等收入国家(LMICs)相关的研究结果。本研究的目的是确定关于听力损失风险因素的系统评价在多大程度上报告了与健康不平等相关的研究结果,以及这些数据在这些系统评价所纳入的原始研究中被记录的程度。
我们从一份关于该主题的报告中识别出关于听力损失风险因素的系统评价,该报告包括对相关系统评价的系统检索。对如此识别出的系统评价,参照PROGRESS-Plus检查与健康不平等相关的数据。我们比较了系统评价与系统评价所纳入的原始研究中数据的报告方式,以及低收入和中等收入国家原始研究的代表性程度。
我们纳入了17项系统评价,这些评价报告了关于听力损失的各种生理、行为、人口统计学和环境风险因素的研究结果。系统评价中包括296项独特的原始研究,其中251项(81.49%)被成功检索到。与健康不平等相关的数据在系统评价中报告得相对较少,主要集中在性别和年龄方面。与健康不平等相关的数据在原始研究中报告得更频繁。然而,几个PROGRESS-Plus标准仅在少数原始研究中被报告。大约三分之一的原始研究来自低收入和中等收入国家。
在关于听力损失风险因素的原始研究中,有改进与健康不平等相关数据报告的空间。然而,系统评价的作者可以做更多工作来报告健康不平等情况,而不是像目前这样,包括梳理出与有数据的低收入和中等收入国家相关的研究结果。