Wang Shun, Zhang Jie, Liu Qiaoli, Deng Liqin
Department of Anesthesiology and Perioperative Medicine, General Hospital of Ningxia Medical University, 804 Shengli Street, Xingqing Area, Yinchuan, Ningxia, China.
Department of Anesthesiology, Clinical Medical College, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, China.
BMC Anesthesiol. 2025 Jun 6;25(1):289. doi: 10.1186/s12871-025-03165-0.
Preoperative oral carbohydrate loading (POCL) has shown benefits in non-diabetic patients, but its use in patients with diabetes remains controversial. Concerns about potential hyperglycemia and adverse outcomes have led to conflicting evidence and varied clinical practices.
To assess the impact of POCL on clinical outcomes after surgery in patients with diabetes.
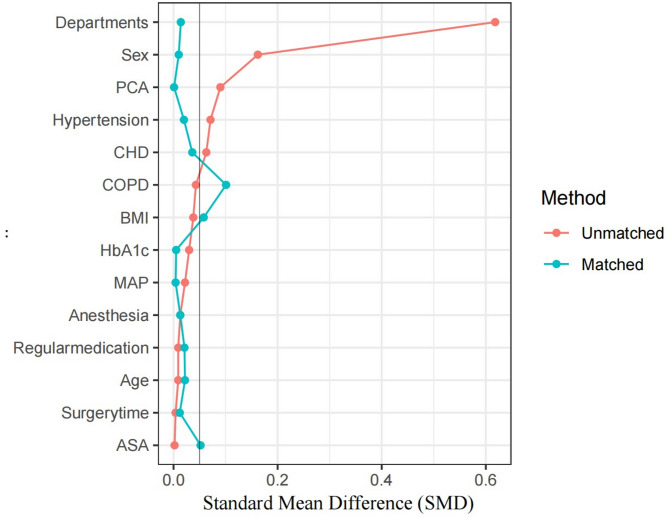
This retrospective study analyzed 679 patients with diabetes undergoing elective surgery from 2020 to 2023, divided into POCL and fasting groups. After 1:1 propensity score matching (PSM), 410 patients were analyzed. Primary outcomes included postoperative blood glucose levels; secondary outcomes were including glycemic variability, pulmonary infections, hospital stay length, and costs.
After PSM, POCL was associated with significantly lower blood glucose levels on the first postoperative day compared to the fasting group (11.03 [9.43–12.77] vs. 11.37 [9.77–13.20], = 0.045). No significant differences were observed in glycemic variability. POCL patients demonstrated shorter postoperative hospital stays (5.10 [3.00-7.70] vs. 5.90 [3.80–8.50], = 0.022). Multivariate analysis revealed that POCL independently predicted reduced hospitalization costs (β=-3417.49, 95% CI [-6358.52, -476.46], = 0.023) and shorter hospital stays (β=-1.21, 95% CI [-1.83, -0.60], < 0.001). Higher ASA scores and longer surgical durations were associated with increased costs, while prolonged surgeries correlated with greater pulmonary infection risk (OR = 1.005, 95% CI [1.003–1.008], < 0.001).
Despite previous concerns, POCL appears to be associated with lower early postoperative blood glucose levels, shorter hospital stays, and reduced costs in patients with well-controlled diabetes (HbA1c < 7.5%). It may be a safe and effective perioperative strategy for this specific population, though individualized assessment remains essential.
术前口服碳水化合物负荷(POCL)已在非糖尿病患者中显示出益处,但其在糖尿病患者中的应用仍存在争议。对潜在高血糖和不良结局的担忧导致了相互矛盾的证据和不同的临床实践。
评估POCL对糖尿病患者术后临床结局的影响。
这项回顾性研究分析了2020年至2023年期间接受择期手术的679例糖尿病患者,分为POCL组和禁食组。经过1:1倾向评分匹配(PSM)后,对410例患者进行了分析。主要结局包括术后血糖水平;次要结局包括血糖变异性、肺部感染、住院时间和费用。
PSM后,与禁食组相比,POCL组术后第一天的血糖水平显著更低(11.03[9.43-12.77]对11.37[9.77-13.20],P=0.045)。血糖变异性方面未观察到显著差异。POCL组患者术后住院时间更短(5.10[3.00-7.70]对5.90[3.80-8.50],P=0.022)。多变量分析显示,POCL独立预测住院费用降低(β=-3417.49,95%CI[-6358.52,-476.46],P=0.023)和住院时间缩短(β=-1.21,95%CI[-1.83,-0.60],P<0.001)。较高的美国麻醉医师协会(ASA)评分和较长的手术时间与费用增加相关,而手术时间延长与肺部感染风险增加相关(OR=1.005,95%CI[1.003-1.008],P<0.001)。
尽管此前存在担忧,但POCL似乎与血糖控制良好(糖化血红蛋白<7.5%)的糖尿病患者术后早期血糖水平降低、住院时间缩短和费用降低相关。对于这一特定人群,它可能是一种安全有效的围手术期策略,不过个体化评估仍然至关重要。