Paz Joaquín De la, Lecaros Juan José, Calvo Andres, Ariztia Antonio, Aravena Cristian, Reinares Felipe
Facultad de Medicina Clínica Alemana, Universidad del Desarrollo, Santiago, Chile.
Hospital Clínico Mutual de Seguridad, Santiago, Chile.
JSES Int. 2024 Dec 13;9(3):878-884. doi: 10.1016/j.jseint.2024.11.019. eCollection 2025 May.
Our understanding of transolecranon fracture dislocation (TOFD) has evolved to include associated ligament, coronoid, and radial head lesions impacting stability, rather than solely bone stability. Similarly, the understanding of coronoid fracture patterns has progressed. O'Driscoll et al state that basal subtype 2 coronoid fractures correspond to a TOFD, with a fracture passing through the base of the coronoid. In the literature, there is no clear differentiation between basal coronoid TOFD (BC-TOFD) and pure-TOFD outcomes. The main objective of this study is to evaluate the functional results and complications of TOFD using a standardized surgical technique. The secondary objectives are to describe the associated injuries and to compare the results between pure-TOFD and BC-TOFD.
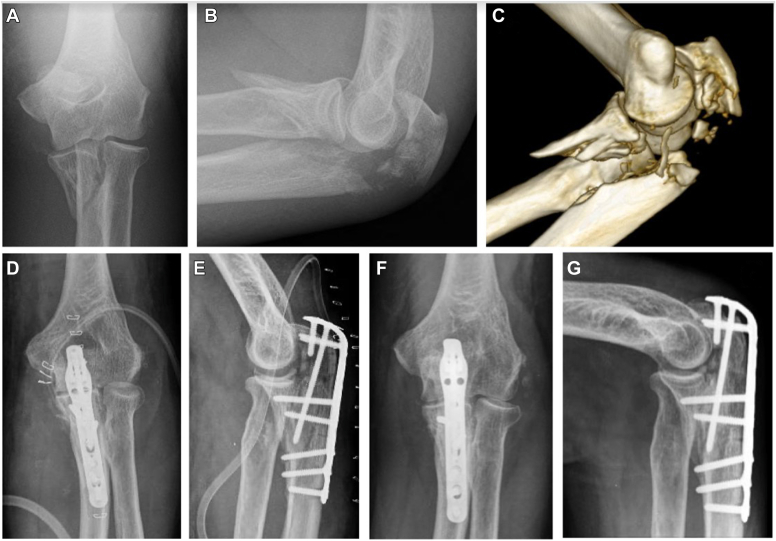
This retrospective study included all patients with a TOFD treated with a standardized surgical procedure and rehabilitation protocol between 2013 and 2018 in a single trauma level 1 center. The surgical procedure mainly consisted of fixing the olecranon with a plate, using the same screws for coronoid fixation and coronoid plate if necessary. Radial head management involved either arthroplasty or screw fixation, with ligament repair performed as needed. Demographic data and the associated bone and ligament injuries were reviewed. The clinical outcomes (range of motion, Mayo Elbow Performance Score (MEPS), and Broberg and Morrey (B&M) scores) were evaluated at the final follow-up, after a minimum of 2 years. Complications and reoperations were assessed.
24 patients were included, and 75.0% were men. The average follow-up was 57.9 ± 22.0 months. The mean age was 42.0 ± 15.1 years. 18 (75.0%) were BC-TOFD and 6 (25.0%) were pure-TOFD. Ligament injuries requiring repair and radial head fracture were present in 8 (33.3%) and 11 (45.8%), respectively. The average range of motion were flexion 119.0° ± 17.6, extension deficit 20.4° ± 12.6°, pronation 68.9° ± 20.4°, and supination 63.1° ± 27.4°. MEPS and B&M mean scores were 82.3 ± 16.5 and 82.0 ± 16.1, respectively. The reoperation rate was 33.3%. No significant differences were found between pure-TOFD and BC-TOFD. A significant distribution difference was found in MEPS ( = .001), B&M ( = .002), range of flexion ( = .011), and extension deficit ( = .005) between patients who had reintervention and those who did not.
A standardized protocol for TOFD allows good to excellent functional results. There are no significant differences between pure-TOFD and BC-TOFD. One-third underwent reintervention. Patients with reintervention presented worse outcomes.
我们对经鹰嘴骨折脱位(TOFD)的认识已有所发展,认识到其相关的韧带、冠状突和桡骨头损伤会影响稳定性,而非仅仅取决于骨骼稳定性。同样,对冠状突骨折类型的认识也有了进展。奥德里斯科尔等人指出,冠状突基底2型骨折相当于经鹰嘴骨折脱位,骨折线穿过冠状突基底。在文献中,冠状突基底经鹰嘴骨折脱位(BC - TOFD)和单纯经鹰嘴骨折脱位的预后并无明确区分。本研究的主要目的是采用标准化手术技术评估经鹰嘴骨折脱位的功能结果及并发症。次要目的是描述相关损伤,并比较单纯经鹰嘴骨折脱位和冠状突基底经鹰嘴骨折脱位的结果。
本回顾性研究纳入了2013年至2018年在单一一级创伤中心接受标准化手术及康复方案治疗的所有经鹰嘴骨折脱位患者。手术主要包括用钢板固定鹰嘴,必要时使用相同螺钉固定冠状突及冠状突钢板。桡骨头处理包括关节成形术或螺钉固定,并根据需要进行韧带修复。回顾了人口统计学数据以及相关的骨骼和韧带损伤情况,并在至少2年的最终随访时评估临床结果(活动范围、梅奥肘关节功能评分(MEPS)以及布罗伯格和莫里(B&M)评分),同时评估并发症和再次手术情况。
纳入24例患者,75.0%为男性。平均随访时间为57.9±22.0个月,平均年龄为42.0±15.1岁。18例(75.0%)为冠状突基底经鹰嘴骨折脱位,6例(25.0%)为单纯经鹰嘴骨折脱位。分别有8例(33.3%)和11例(45.8%)存在需要修复的韧带损伤和桡骨头骨折。平均活动范围为:屈曲119.0°±17.6°,伸展受限20.4°±12.6°,旋前68.9°±20.4°,旋后63.1°±27.4°。MEPS和B&M平均评分分别为82.3±16.5和82.0±16.1。再次手术率为33.3%。单纯经鹰嘴骨折脱位和冠状突基底经鹰嘴骨折脱位之间未发现显著差异。在再次干预患者和未再次干预患者之间,MEPS(P = 0.001)、B&M(P = 0.002)、屈曲范围(P = 0.011)和伸展受限(P = 0.005)方面存在显著分布差异。
经鹰嘴骨折脱位的标准化方案可取得良好至优异的功能结果。单纯经鹰嘴骨折脱位和冠状突基底经鹰嘴骨折脱位之间无显著差异。三分之一的患者接受了再次干预。接受再次干预的患者预后较差。