Louca Antros, Petursson Petur, Sundström Joakim, Rawshani Araz, Hagström Henrik, Settergren Magnus, James Stefan, Koul Sasha, Skoglund Kristofer, Ioanes Dan, Völz Sebastian, Myredal Anna, Angerås Oskar, Råmunddal Truls
Department of Cardiology Sahlgrenska University Hospital, Gothenburg, Sweden.
Department of Molecular and Clinical Medicine, Institute of Medicine, University of Gothenburg, Gothenburg, Sweden.
Int J Cardiol Heart Vasc. 2025 May 14;59:101705. doi: 10.1016/j.ijcha.2025.101705. eCollection 2025 Aug.
Limited data exist on transcatheter aortic valve replacement (TAVR) outcomes in patients with bicuspid aortic valve (BAV) stenosis. This study compared TAVR outcomes in BAV versus tricuspid aortic stenosis.
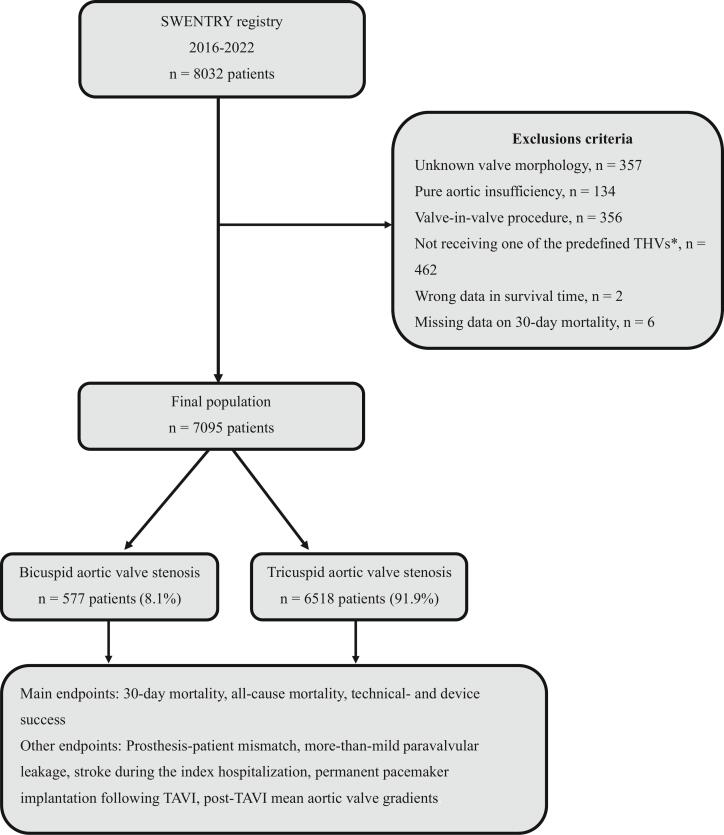
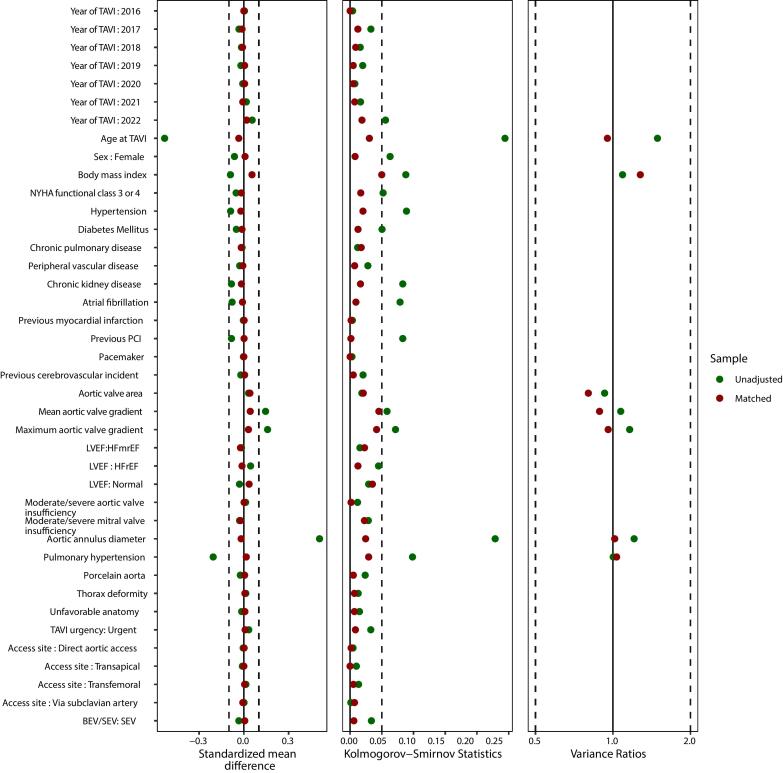
This observational study included all patients who underwent TAVR in Sweden from 2016 to 2022, excluding those with pure aortic insufficiency and valve-in-valve procedures. Only Evolut-, SAPIEN-, ACURATE-, and Portico/Navitor-family devices were included. A doubly robust method was used, combining propensity score estimation and multivariable regression.
Among 7,095 patients, 577 (8.1 %) had BAV stenosis. The mean EUROSCORE II-predicted mortality risk was 3.8 % for BAV and 4.5 % for TAV. BAV patients were younger, predominantly male, and had fewer comorbidities but higher baseline aortic valve gradients, larger annulus diameters, and more reduced ejection fraction.After matching, 30-day mortality and all-cause mortality (median follow-up: 690 days) were similar between BAV and TAV patients (p = 0.8 for both). While BAVs had numerically lower technical success per VARC-3 criteria, this was not statistically significant (p = 0.08). However, BAV patients had lower device success (aOR = 0.8, p = 0.04) and a higher incidence of post-TAVR pacemaker implantation (aOR = 1.76, 95 % CI: 1.14-2.58, p = 0.007). No significant differences were observed in prosthesis-patient mismatch (p = 0.3), paravalvular leakage (p = 0.6), stroke (p = 0.3), or post-TAVR gradients (p > 0.9).
TAVR in BAV patients yields similar mortality and hemodynamic outcomes as in TAV patients. However, BAVs are associated with lower device success and higher pacemaker rates. While TAVR is a viable alternative to SAVR, treatment should be individualized, especially in younger BAV patients, considering lifetime management and coronary access.
关于经导管主动脉瓣置换术(TAVR)治疗二叶式主动脉瓣(BAV)狭窄患者的预后数据有限。本研究比较了BAV与三叶式主动脉瓣狭窄患者的TAVR预后。
这项观察性研究纳入了2016年至2022年在瑞典接受TAVR的所有患者,排除了单纯主动脉瓣关闭不全患者和瓣中瓣手术患者。仅纳入Evolut、SAPIEN、ACURATE和Portico/Navitor系列器械。采用双重稳健方法,结合倾向评分估计和多变量回归。
在7095例患者中,577例(8.1%)患有BAV狭窄。BAV患者的欧洲心脏手术风险评估系统(EUROSCORE)II预测死亡率平均为3.8%,三叶式主动脉瓣(TAV)患者为4.5%。BAV患者更年轻,以男性为主,合并症较少,但基线主动脉瓣压力阶差更高,瓣环直径更大,射血分数降低更明显。匹配后,BAV和TAV患者的30天死亡率和全因死亡率(中位随访时间:690天)相似(两者p = 0.8)。虽然根据VARC-3标准,BAV患者的技术成功率在数值上较低,但无统计学意义(p = 0.08)。然而,BAV患者的器械成功率较低(调整后比值比[aOR]=0.8,p = 0.04),TAVR术后起搏器植入发生率较高(aOR = 1.76,95%可信区间:1.14 - 2.58,p = 0.007)。在人工瓣膜-患者不匹配(p = 0.3)、瓣周漏(p = 0.6)、卒中(p = 0.3)或TAVR术后压力阶差(p > 0.9)方面未观察到显著差异。
BAV患者的TAVR死亡率和血流动力学结果与TAV患者相似。然而,BAV与较低的器械成功率和较高的起搏器植入率相关。虽然TAVR是外科主动脉瓣置换术(SAVR)的可行替代方案,但治疗应个体化,尤其是年轻的BAV患者,需考虑终身管理和冠状动脉通路。