Hou Cunpeng, Zhang Yaqi, Zhao Feiyang, Lv Yanling, Luo Mengyun, Pan Chensheng, Ding Ding, Chen Liangkai
Department of Nutrition and Food Hygiene, Hubei Key Laboratory of Food Nutrition and Safety, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Ministry of Education Key Lab of Environment and Health, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
JAMA Netw Open. 2025 Jun 2;8(6):e2514316. doi: 10.1001/jamanetworkopen.2025.14316.
Active travel modes, such as walking and cycling, are feasible and readily embraced forms of physical activity, but their association with dementia risk and brain structure remains unclear.
To investigate the long-term association between travel modes and dementia risk and brain structural metrics and to evaluate whether genetic predisposition could modify the association between travel modes and dementia risk.
DESIGN, SETTING, AND PARTICIPANTS: This prospective cohort study included data collected from the UK Biobank from March 13, 2006, to October 1, 2010. Data were analyzed from March to October 2024.
Travel modes assessed using the question "In the last 4 weeks, which forms of transport have you used most often to get about (not including any journeys to and from work)?" and categorized into 4 groups: nonactive, walking, mixed-walking, and cycling and mixed-cycling mode.
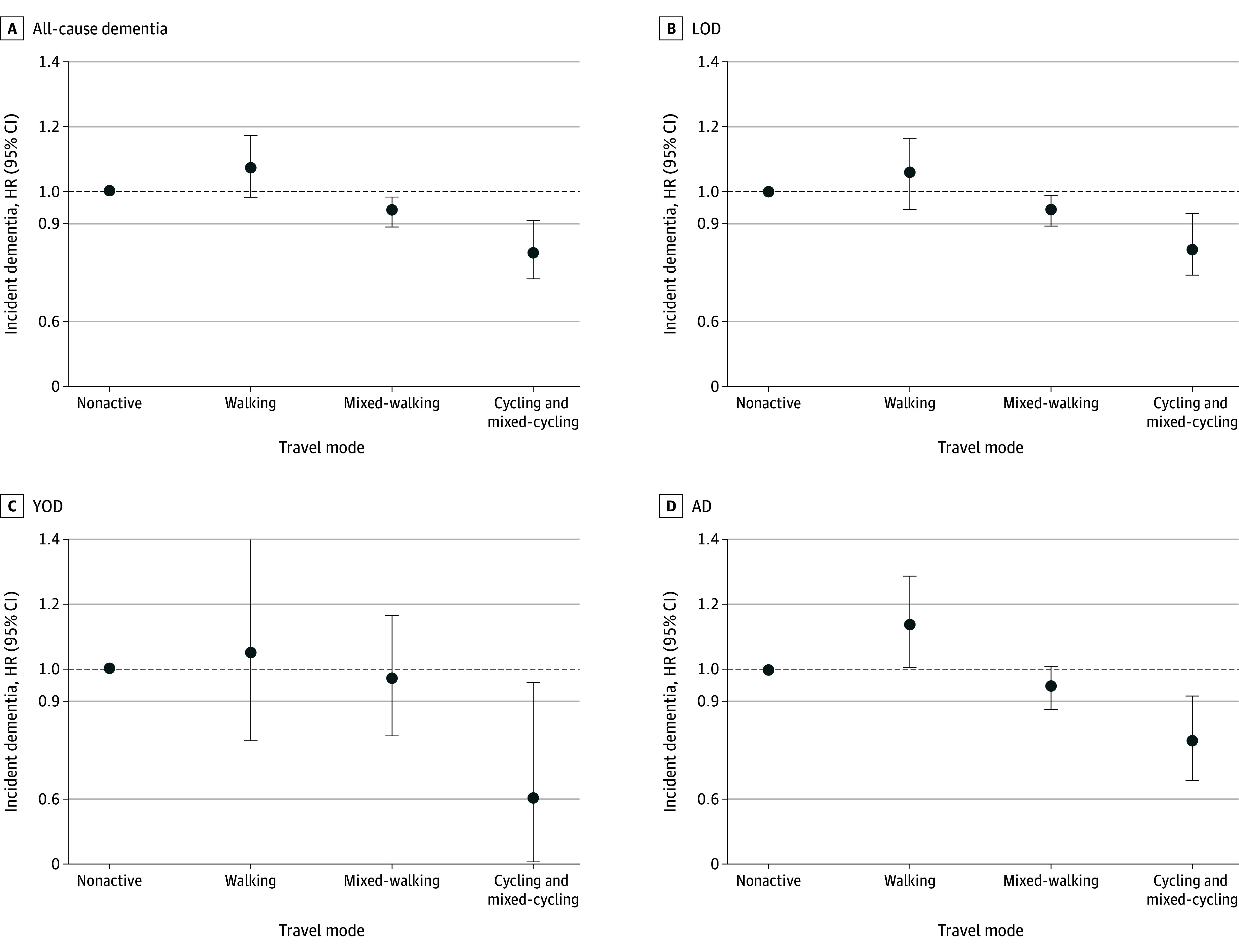
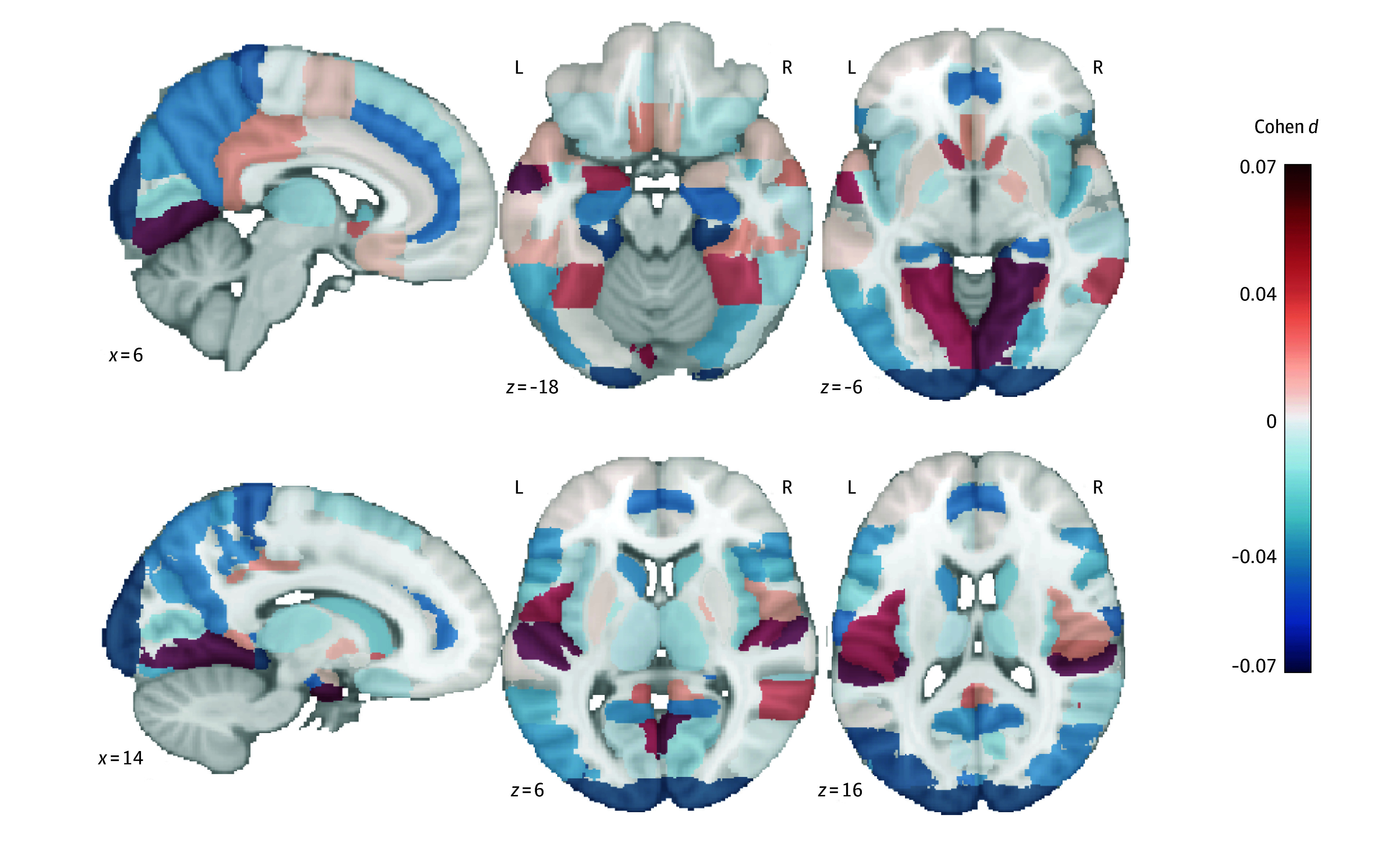
The incidence of all-cause dementia (including young-onset dementia [YOD] and late-onset dementia [LOD]) was the primary outcome, and dementia subtypes, such as Alzheimer disease (AD) and brain structure, were the secondary outcomes; all were identified through hospital records and death registers. Brain structure was measured by a magnetic resonance imaging scan. Travel mode and risk of incident dementia were assessed using Cox proportional hazards regression models with hazard ratios and 95% CIs.
The study encompassed 479 723 participants (mean [SD] age, 56.5 [8.1] years; 260 730 females [54.4%]), including 271 690 in the YOD analyses and 334 939 in the LOD analyses. Over a median follow-up of 13.1 years (IQR, 12.8-13.5 years), 8845 cases of dementia (1.8%) and 3956 cases of AD (0.8%) were recorded. Compared with a nonactive travel mode, multivariable-adjusted hazard ratios for cycling and mixed-cycling were 0.81 (95% CI, 0.73-0.91) for all-cause dementia, 0.78 (95% CI, 0.66-0.92) for AD, 0.60 (95% CI, 0.38-0.95) for YOD, and 0.83 (95% CI, 0.75-0.93) for LOD. A significant interaction between travel mode and genetic susceptibility in the all-cause dementia analysis (P = .02 for interaction) and the LOD analysis (P = .04 for interaction) was observed; specifically, for the cycling and mixed-cycling groups, the risks of all-cause dementia and LOD were lower among those without apolipoprotein E ε4 (APOE ε4) carrier status (all-cause dementia: hazard ratio [HR], 0.74 [95% CI, 0.63-0.87]; LOD: HR, 0.75 [95% CI, 0.63-0.89]) compared with those with APOE ε4 carrier status (all-cause dementia: HR, 0.88 [95% CI, 0.76-1.02]; LOD: HR, 0.91 [95% CI, 0.78-1.05]). The cycling and mixed-cycling mode was significantly associated with a higher hippocampal volume (β, 0.05 [95% CI, 0.02-0.08]). Genetic risk significantly modified the association with all-cause dementia (P = .02 for interaction) and LOD (P = .04 for interaction). Specifically, for the cycling and mixed-cycling groups, the risk of all-cause dementia was lower among those without APOE ε4 (HR, 0.74 [95% CI, 0.63-0.87]) compared with those with APOE ε4 (HR, 0.88 [95% CI, 0.76-1.02]). Similarly, the risk of LOD was lower among those without APOE ε4 (HR, 0.75 [95% CI, 0.63-0.89]) compared with those with APOE ε4 (HR, 0.91 [95% CI, 0.78-1.05]).
The findings of this cohort study suggest an association between active travel mode and incident dementia and brain structure. The cycling and mixed-cycling mode was associated with a reduced risk of all-cause dementia, including YOD, LOD, and AD, as well as an increased hippocampal volume, suggesting a promising approach for maintaining brain health.
步行和骑自行车等主动出行方式是可行且容易接受的身体活动形式,但其与痴呆症风险和脑结构之间的关联仍不明确。
研究出行方式与痴呆症风险及脑结构指标之间的长期关联,并评估遗传易感性是否会改变出行方式与痴呆症风险之间的关联。
设计、背景和参与者:这项前瞻性队列研究纳入了2006年3月13日至2010年10月1日从英国生物银行收集的数据。数据于2024年3月至10月进行分析。
使用“在过去4周内,您最常使用哪种交通方式出行(不包括上下班行程)?”这一问题评估出行方式,并分为4组:非主动出行、步行、步行与其他混合、骑自行车与其他混合出行模式。
全因痴呆症(包括早发性痴呆症[YOD]和晚发性痴呆症[LOD])的发病率是主要结局,痴呆症亚型,如阿尔茨海默病(AD)和脑结构是次要结局;所有结局均通过医院记录和死亡登记确定。脑结构通过磁共振成像扫描测量。使用Cox比例风险回归模型评估出行方式与痴呆症发病风险,得出风险比和95%置信区间。
该研究纳入了479723名参与者(平均[标准差]年龄为56.5[8.1]岁;260730名女性[54.4%]),其中YOD分析中有271690名参与者,LOD分析中有334939名参与者。在中位随访13.1年(四分位间距为12.8 - 13.5年)期间,记录了8845例痴呆症病例(占1.8%)和3956例AD病例(占0.8%)。与非主动出行模式相比,多变量调整后的骑自行车与其他混合出行模式的全因痴呆症风险比为0.81(95%置信区间为0.73 - 0.91),AD为0.78(95%置信区间为0.66 - 0.92),YOD为0.60(95%置信区间为0.38 - 0.95),LOD为0.83(95%置信区间为0.75 - 0.93)。在全因痴呆症分析(交互作用P = 0.02)和LOD分析(交互作用P = 0.04)中观察到出行方式与遗传易感性之间存在显著交互作用;具体而言,对于骑自行车与其他混合出行组,无载脂蛋白E ε4(APOE ε4)携带者状态的人群中全因痴呆症和LOD的风险低于有APOE ε4携带者状态的人群(全因痴呆症:风险比[HR]为0.74[95%置信区间为0.63 - 0.87];LOD:HR为0.75[95%置信区间为0.63 - 0.89]),而有APOE ε4携带者状态的人群中全因痴呆症风险比为0.88(95%置信区间为0.76 - 1.02);LOD风险比为0.91(95%置信区间为0.78 - 1.05)。骑自行车与其他混合出行模式与较高的海马体体积显著相关(β值为0.05[95%置信区间为0.02 - 0.08])。遗传风险显著改变了与全因痴呆症(交互作用P = 0.02)和LOD(交互作用P = 0.04)的关联。具体而言,对于骑自行车与其他混合出行组,无APOE ε4的人群中全因痴呆症风险低于有APOE ε4的人群(HR为0.74[95%置信区间为0.63 - 0.87])。同样,无APOE ε4的人群中LOD风险低于有APOE ε4的人群(HR为0.75[95%置信区间为0.63 - 0.89]),而有APOE ε4的人群中LOD风险比为0.91(95%置信区间为0.78 - 1.05)。
这项队列研究的结果表明主动出行方式与痴呆症发病及脑结构之间存在关联。骑自行车与其他混合出行模式与全因痴呆症风险降低相关,包括YOD、LOD和AD,同时海马体体积增加,这表明这是一种维护脑健康的有前景的方法。