Obeidat Khaled A, Saadeh Nesreen A, Msameh Renad, Obeidat Ajwad, Mar'ey Omar, Bakkar Ahmad, Manasrah Qutaiba
Department of Surgery, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan.
Department of Medicine, Faculty of Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan.
Endocrinol Diabetes Metab. 2025 Jul;8(4):e70070. doi: 10.1002/edm2.70070.
Hypocalcemia is a common event after parathyroidectomy for primary hyperparathyroidism (PHPT). This study aimed to explore the incidence of hypocalcemia, determine risk factors, and identify serum biomarkers associated with the development of this condition.
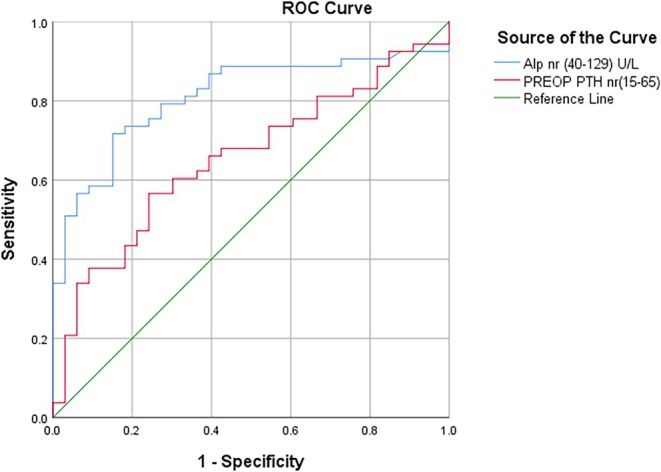
A retrospective study that included 116 patients with PHPT who underwent parathyroidectomy at a tertiary care facility in Jordan over 16 years (2006-2022) in this study. Patients were classified as having postoperative hypocalcemia if they developed serum calcium levels < 2.15 mmol/L within the first week following parathyroidectomy. Logistic regression analysis was performed to determine predictors of hypocalcemia. Spearman's rank correlation coefficient and ROC curves were used to assess relationships between variables as well as determine cutoffs for these predictors.
Of the 116 patients studied, 57.7% developed hypocalcemia after parathyroidectomy. High preoperative alkaline phosphatase (ALP), low preoperative corrected calcium, high preoperative parathyroid (PTH), and younger age were shown to be significantly higher in patients who developed hypocalcemia after parathyroidectomy. Multivariate logistic regression showed a low preoperative corrected calcium level was an independent predictor of postoperative hypocalcemia (p = 0.036). A high level of preoperative alkaline phosphatase was also considered an independent predictor of hypocalcemia development (OR = 1.007, 95% CI: 1.002-1.012). Patients who had pre-operative ALP less than 208.5 U/L were unlikely to develop postoperative hypocalcemia.
Our study identified higher preoperative ALP, lower pre-operative corrected calcium, higher pre-operative PTH levels, and younger age as risk factors for postoperative hypocalcemia. Preoperative ALP and preoperative corrected calcium were shown to be independent predictors of hypocalcemia development.
甲状旁腺切除术后发生低钙血症是原发性甲状旁腺功能亢进症(PHPT)常见的情况。本研究旨在探讨低钙血症的发生率,确定危险因素,并识别与该病症发生相关的血清生物标志物。
本研究为一项回顾性研究,纳入了16年间(2006 - 2022年)在约旦一家三级医疗机构接受甲状旁腺切除术的116例PHPT患者。如果患者在甲状旁腺切除术后第一周内血清钙水平<2.15 mmol/L,则被分类为术后低钙血症。进行逻辑回归分析以确定低钙血症的预测因素。使用Spearman等级相关系数和ROC曲线来评估变量之间的关系以及确定这些预测因素的临界值。
在研究的116例患者中,57.7%在甲状旁腺切除术后发生低钙血症。甲状旁腺切除术后发生低钙血症的患者术前碱性磷酸酶(ALP)高、术前校正钙低、术前甲状旁腺素(PTH)高以及年龄较小的情况显著更多。多因素逻辑回归显示术前校正钙水平低是术后低钙血症的独立预测因素(p = 0.036)。术前碱性磷酸酶水平高也被认为是低钙血症发生的独立预测因素(OR = 1.007,95% CI:1.002 - 1.012)。术前ALP低于208.5 U/L的患者不太可能发生术后低钙血症。
我们的研究确定术前ALP较高、术前校正钙较低、术前PTH水平较高以及年龄较小是术后低钙血症的危险因素。术前ALP和术前校正钙被证明是低钙血症发生的独立预测因素。