Huang Ziyu, Jiang Bailin, Zhao Hong, Feng Yi
Department of Anesthesiology, Peking University People's Hospital, Beijing, China.
Department of Pain Medicine, Peking University People's Hospital, Beijing, China.
Transl Pediatr. 2025 May 30;14(5):1033-1038. doi: 10.21037/tp-2024-607. Epub 2025 May 16.
Bronchiolitis obliterans syndrome (BOS) is a rare but severe noninfectious pulmonary complication that typically arises in the context of chronic graft-versus-host disease (cGVHD) following allogeneic hematopoietic stem cell transplantation (HSCT). Characterized by progressive small airflow obstruction and irreversible airflow limitation, it poses significant challenges in managing general anesthesia, especially in pediatric patients. There is currently no established consensus or clinical research on the optimal anesthetic approach for such cases, making this report noteworthy.
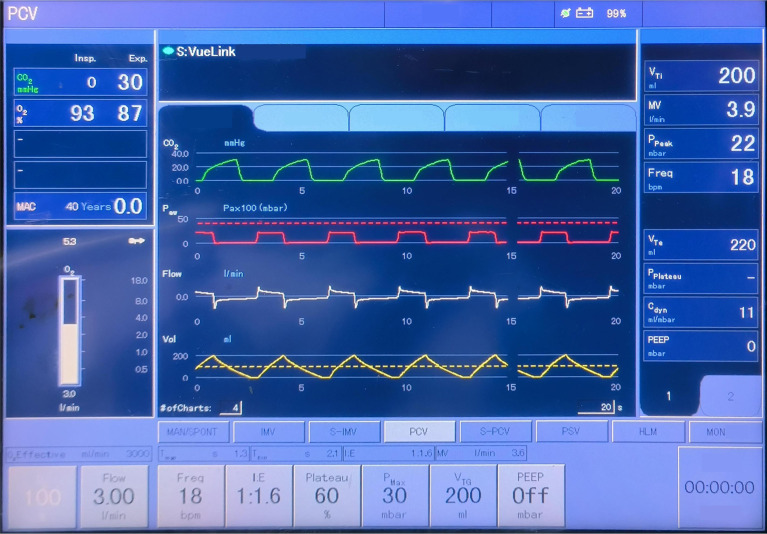
We report the case of a 6-year-old boy with BOS and steroid-induced obesity who had undergone HSCT for acute lymphoblastic leukemia and required general anesthesia for cataract surgery. He had severely reduced lung function and hypercapnia. Anesthesia was induced with propofol, rocuronium, and remifentanil, and mechanical ventilation was managed using pressure-controlled ventilation-volume guaranteed (PCV-VG) mode to minimize airway pressures and prevent barotrauma. The surgery was completed without complications, and the patient was safely extubated and discharged the next day.
This case demonstrates that the PCV-VG ventilation mode can be a viable option for managing pediatric patients with severe BOS undergoing general anesthesia. This approach can help achieve sufficient ventilation while minimizing airway pressures and the risk of ventilator-induced lung injury. This approach offers a viable anesthetic management option for similar cases in the future.
闭塞性细支气管炎综合征(BOS)是一种罕见但严重的非感染性肺部并发症,通常发生在异基因造血干细胞移植(HSCT)后的慢性移植物抗宿主病(cGVHD)背景下。其特征为进行性小气道阻塞和不可逆的气流受限,在全身麻醉管理中带来重大挑战,尤其是在儿科患者中。目前对于此类病例的最佳麻醉方法尚无既定的共识或临床研究,因此本报告具有重要意义。
我们报告一例6岁患有BOS和类固醇诱导性肥胖的男孩,他因急性淋巴细胞白血病接受了HSCT,白内障手术需要全身麻醉。他的肺功能严重下降且存在高碳酸血症。采用丙泊酚、罗库溴铵和瑞芬太尼诱导麻醉,并使用压力控制通气-容量保证(PCV-VG)模式进行机械通气,以尽量降低气道压力并防止气压伤。手术顺利完成,无并发症发生,患者于次日安全拔管并出院。
本病例表明,PCV-VG通气模式对于患有严重BOS的儿科患者进行全身麻醉管理可能是一种可行的选择。这种方法有助于在尽量降低气道压力和呼吸机诱导性肺损伤风险的同时实现充分通气。该方法为未来类似病例提供了一种可行的麻醉管理选择。