He Chunlei, Yuan Enyu, Ye Lei, Xu Hui, Zhang Xiaoyong, Zeng Hao, Chen Yuntian, Yao Jin, Song Bin
Department of Radiology, West China Hospital, Sichuan University, Chengdu, China.
Department of Radiology, Sanya People's Hospital, Sanya, China.
Korean J Radiol. 2025 Jul;26(7):678-687. doi: 10.3348/kjr.2024.1202. Epub 2025 Jun 13.
To investigate the feasibility of time-dependent diffusion-weighted imaging (-) in assessing the pathological World Health Organization/International Society of Urological Pathology (WHO/ISUP) grade of clear cell renal cell carcinoma (ccRCC).
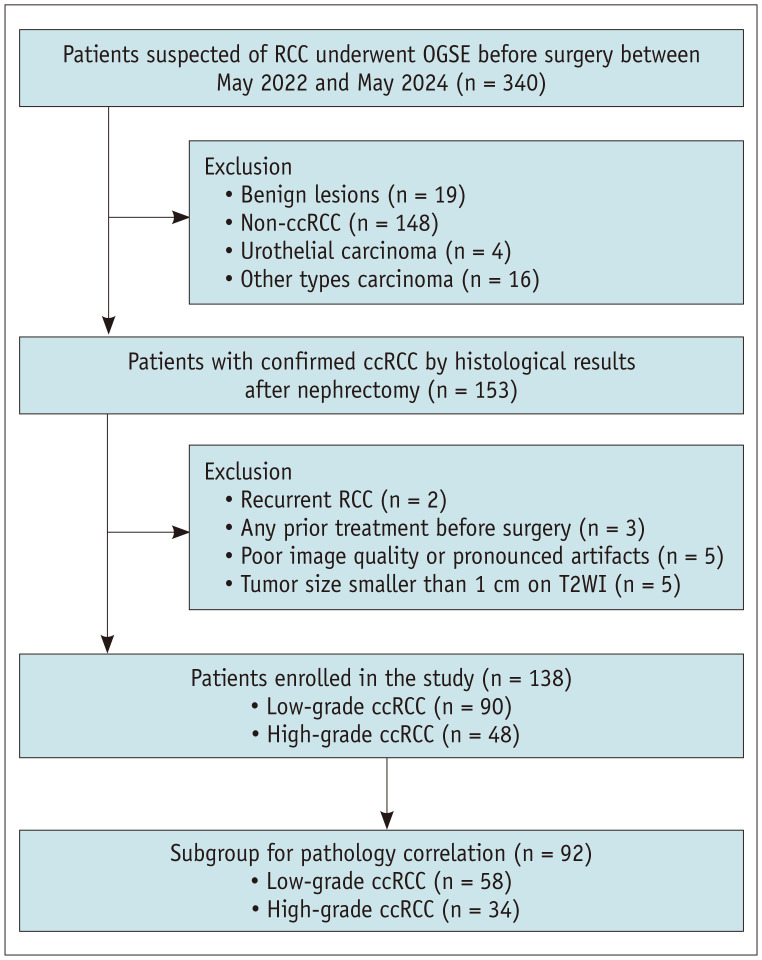
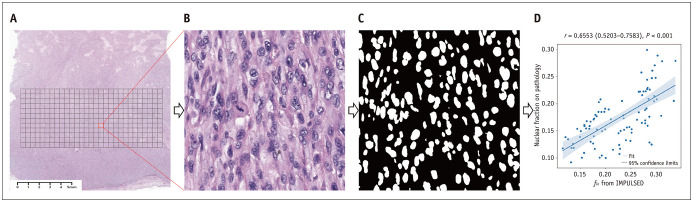
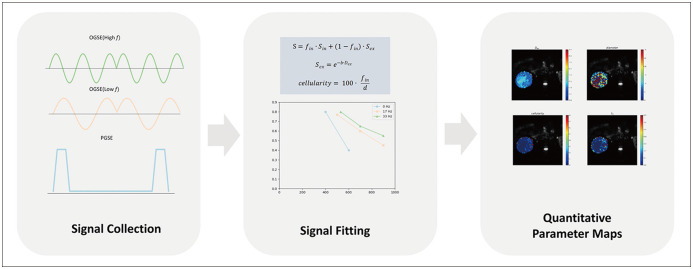
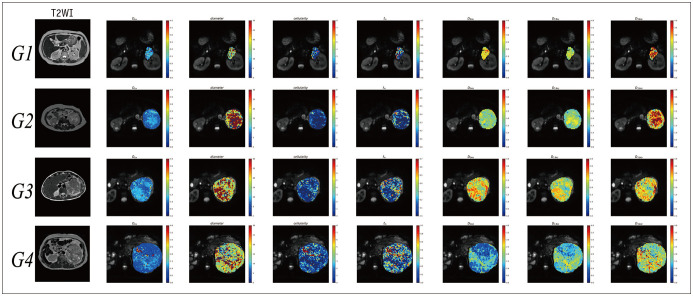
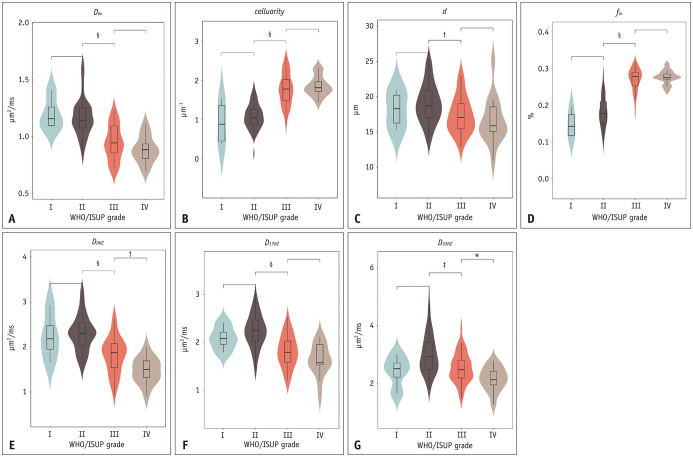
A total of 138 patients (median age, 58 years [interquartile range, 51-64 years]; 89 males) with surgically confirmed ccRCC, comprising 48 high-grade (WHO/ISUP grade III/IV) and 90 low-grade (WHO/ISUP grade I/II) tumors, were included in the study among patients who underwent preoperative - for suspected RCC between May 2022 and May 2024. The - microstructural parameters, including cell (), intracellular volume fraction (), , and extracellular diffusivities (), were quantified using a two-compartment model. The solid tumor area was manually annotated to extract the mean values from each parameter map. We analyzed the differences in - parameters between the high- and low-grade tumors and evaluated the ability of these parameters to distinguish between the two tumor groups. High-definition hematoxylin-and-eosin-stained slides were obtained from 92 patients. We assessed the correlation between - parameters and pathologic nuclear fraction, which was quantified using an automated nucleus segmentation model (Hover-Net).
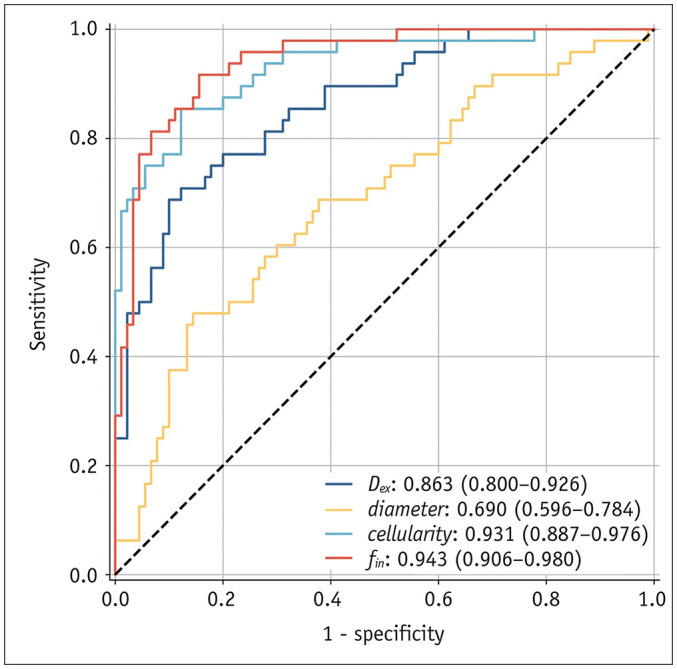
Compared to high-grade tumors, low-grade tumors exhibited lower and and higher and . For differentiation between low- and high-grade ccRCC, the exhibited the highest diagnostic performance (areas under the receiver operating characteristic curve [AUC] = 0.943; 95% confidence interval, 0.906-0.980), followed by (AUC = 0.931; 0.887-0.976), (AUC = 0.863; 0.800-0.926), and (AUC = 0.690; 0.596-0.784). The nuclei on pathology slides were automatically segmented, and the nuclear fraction exhibited a moderate correlation with ( = 0.65, < 0.001).
探讨时间依赖扩散加权成像(-)评估透明细胞肾细胞癌(ccRCC)的世界卫生组织/国际泌尿病理学会(WHO/ISUP)病理分级的可行性。
2022年5月至2024年5月期间,对138例经手术确诊为ccRCC的患者(中位年龄58岁[四分位间距,51 - 64岁];89例男性)进行了研究,其中包括48例高级别(WHO/ISUP III/IV级)和90例低级别(WHO/ISUP I/II级)肿瘤。这些患者因疑似肾细胞癌接受了术前-。使用双室模型对-微观结构参数进行量化,包括细胞()、细胞内体积分数()、,和细胞外扩散率()。手动标注实体瘤区域以从每个参数图中提取平均值。我们分析了高级别和低级别肿瘤之间-参数的差异,并评估了这些参数区分两组肿瘤的能力。从92例患者中获取了高清苏木精-伊红染色切片。我们评估了-参数与病理核分数之间的相关性,病理核分数使用自动核分割模型(Hover-Net)进行量化。
与高级别肿瘤相比,低级别肿瘤的和较低,而和较高。对于低级别和高级别ccRCC的鉴别,表现出最高的诊断性能(受试者操作特征曲线下面积[AUC] = 0.943;95%置信区间,0.906 - 0.980),其次是(AUC = 0.931;0.887 - 0.976)、(AUC = 0.863;0.800 - 0.926)和(AUC = 0.690;0.596 - 0.784)。病理切片上的细胞核被自动分割,核分数与呈中度相关(= 0.65,< 0.001)。
-参数显示出评估WHO/ISUP病理分级的潜力,可能成为表征肾细胞癌的有前景的非侵入性生物标志物。